

Dynamic changes of angiopoietins and endothelial nitric oxide supply during fluid resuscitation for major gyn-oncological surgery: a prospective observation
- PMID: 32005259
- PMCID: PMC6995240
- DOI: 10.1186/s12967-020-02236-9
Dynamic changes of angiopoietins and endothelial nitric oxide supply during fluid resuscitation for major gyn-oncological surgery: a prospective observation
Abstract
Background: Despite goal-directed hemodynamic therapy, vascular function may deteriorate during surgery for advanced abdominal tumor masses. Fluid administration has been shown to be associated with distinct changes in serum levels of functional proteins. We sought to determine how serum total protein and angiopoietin (ANG) levels change during major abdominal tumor surgery. In addition, ex vivo endothelial nitric oxide synthase (eNOS) activation as well as NO bioavailability in vivo were assessed.
Methods: 30 patients scheduled for laparotomy for late-stage ovarian or uterine cancer were prospectively included. Advanced hemodynamic monitoring as well as protocol-driven goal-directed fluid optimization were performed. Total serum protein, ANG-1, -2, and soluble TIE2 were determined pre-, intra-, and postoperatively. Phosphorylation of eNOS was assessed in microvascular endothelial cells after incubation with patient serum, and microvascular reactivity was determined in vivo by near-infrared spectroscopy and arterial vascular occlusion.
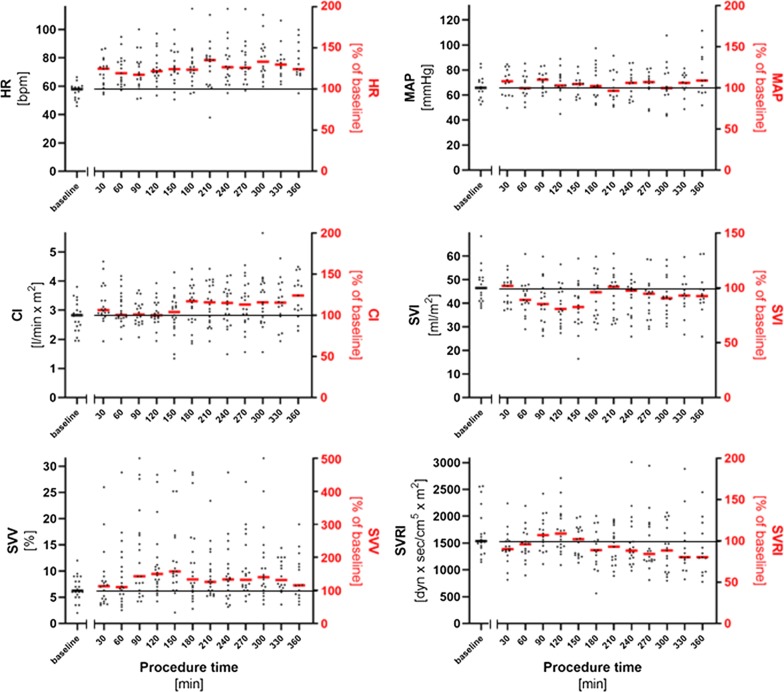
Results: Cardiac output as well as preload gradually decreased during surgery and were associated with a median total fluid intake of 12.8 (9.7-15.4) mL/kg*h and a postoperative fluid balance of 6710 (4113-9271) mL. Total serum protein decreased significantly from baseline (66.5 (56.4-73.3) mg/mL) by almost half intraoperatively (42.7 (36.8-51.5) mg/mL, p < 0.0001) and remained at low level. While ANG-1 showed no significant dilutional change (baseline: 12.7 (11.9-13.9) ng/mL, postop.: 11.6 (10.8 -13.5) ng/mL, p = 0.06), serum levels of ANG-2 were even increased postoperatively (baseline: 2.2 (1.6-2.6) ng/mL vs. postop.: 3.4 (2.3-3.8) ng/mL, p < 0.0001), resulting in a significant shift in ANG-2 to ANG-1 ratio. Ex vivo phosphorylation of eNOS was decreased depending on increased ANG-2 levels and ANG-2/1 ratio (Spearman r = - 0.37, p = 0.007). In vivo, increased ANG-2 levels were associated with impaired capillary recruitment and NO bioavailability (Spearman r = - 0.83, p = 0.01).
Conclusions: Fluid resuscitation-associated changes in serum vascular mediator profile during abdominal tumor surgery were accompanied by impaired eNOS activity ex vivo as well as reduced NO bioavailability in vivo. Our results may explain disturbed microvascular function in major surgery despite goal-directed hemodynamic optimization.
Keywords: Angiopoietins; Fluid resuscitation; Microvascular reactivity; Nitric oxide; eNOS.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Feldheiser A, Hunsicker O, Kaufner L, Köhler J, Sieglitz H, Casans Francés R, et al. Dynamic muscle O2 saturation response is impaired during major non-cardiac surgery despite goal-directed haemodynamic therapy. Rev Esp Anestesiol Reanim. 2016;63:149–158. doi: 10.1016/j.redar.2015.06.011. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
