

Dose-escalation trial of budesonide in surfactant for prevention of bronchopulmonary dysplasia in extremely low gestational age high-risk newborns (SASSIE)
- PMID: 32006953
- PMCID: PMC7223897
- DOI: 10.1038/s41390-020-0792-y
Dose-escalation trial of budesonide in surfactant for prevention of bronchopulmonary dysplasia in extremely low gestational age high-risk newborns (SASSIE)
Abstract
Background: Initial trials of lung-targeted budesonide (0.25 mg/kg) in surfactant to prevent bronchopulmonary dysplasia (BPD) in premature infants have shown benefit; however, the optimal safe dose is unknown.
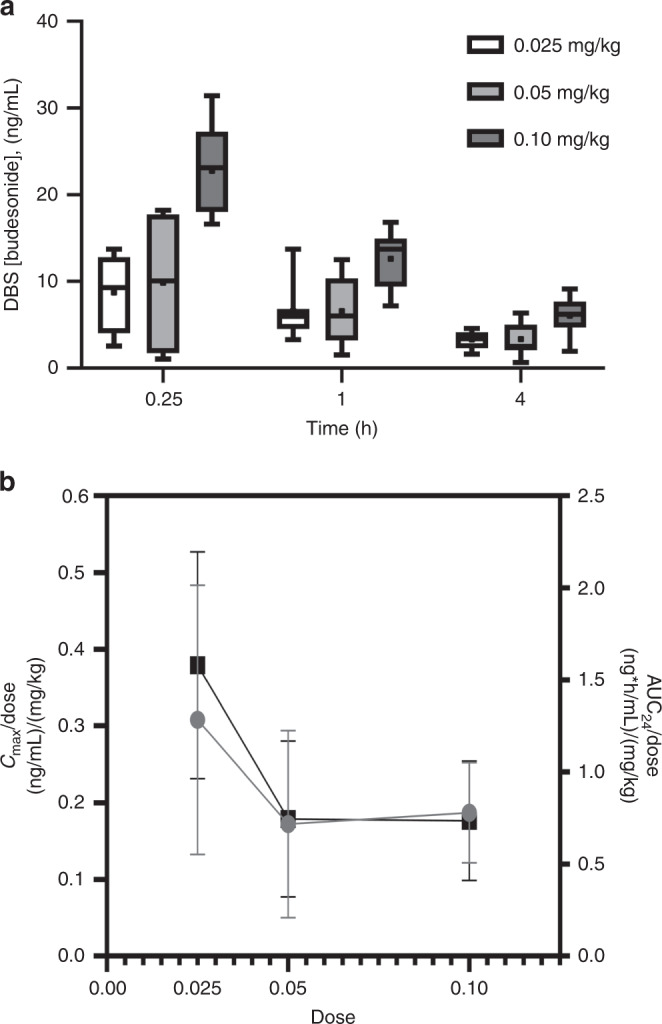
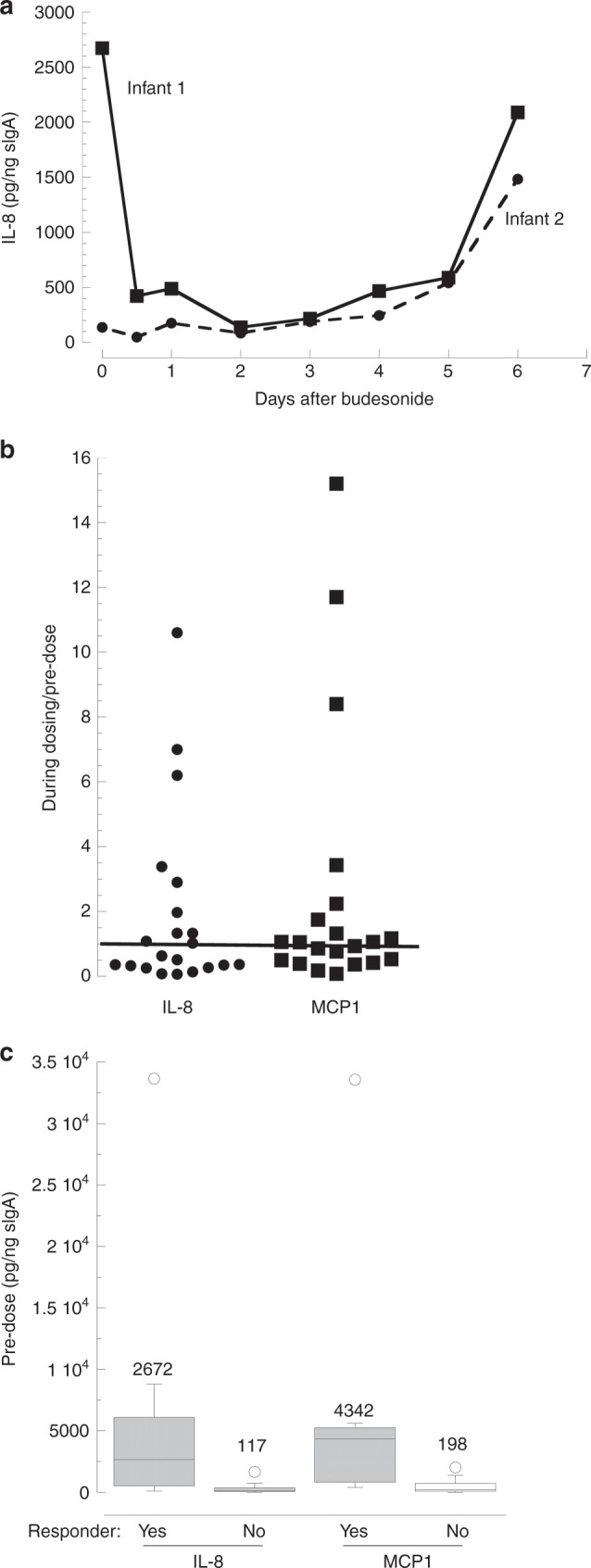
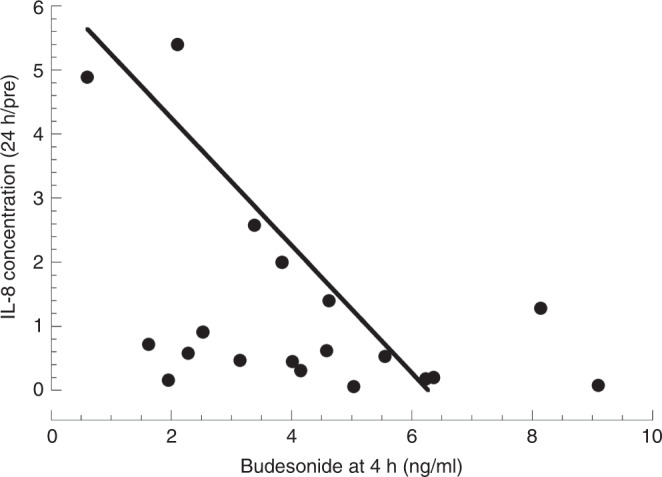
Methods: Dose-escalation study of budesonide (0.025, 0.05, 0.10 mg/kg) in calfactatant in extremely low gestational age neonates (ELGANs) requiring intubation at 3-14 days. Tracheal aspirate (TA) cytokines, blood budesonide concentrations, and untargeted blood metabolomics were measured. Outcomes were compared with matched infants receiving surfactant in the Trial Of Late SURFactant (TOLSURF).
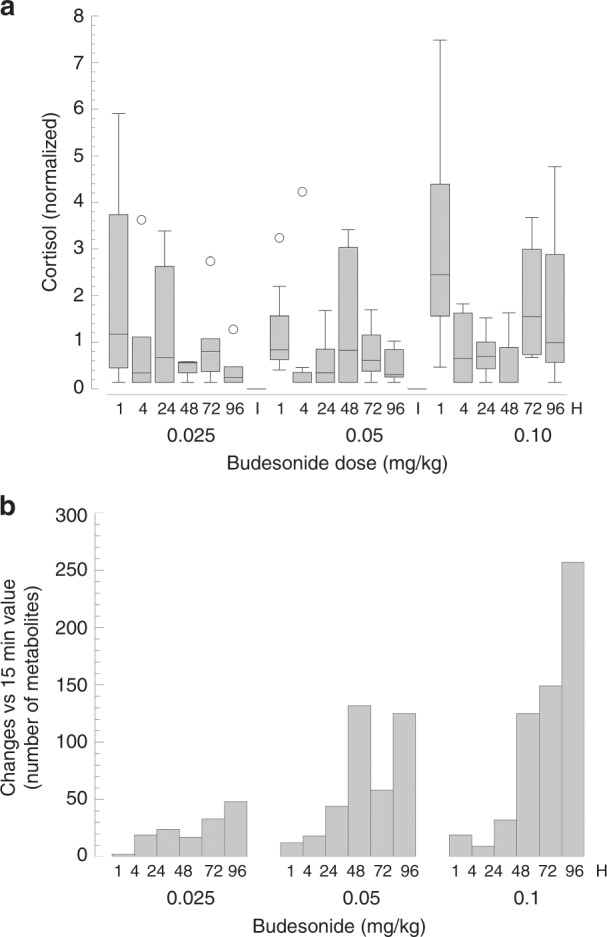
Results: Twenty-four infants with mean gestational age 25.0 weeks and 743 g birth weight requiring mechanical ventilation were enrolled at mean age 6 days. Budesonide was detected in the blood of all infants with a half-life of 3.4 h. Of 11 infants with elevated TA cytokine levels at baseline, treatment was associated with sustained decrease (mean 65%) at all three dosing levels. There were time- and dose-dependent decreases in blood cortisol concentrations and changes in total blood metabolites. Respiratory outcomes did not differ from the historic controls.
Conclusions: Budesonide/surfactant had no clinical respiratory benefit at any dosing levels for intubated ELGANs. One-tenth the dose used in previous trials had minimal systemic metabolic effects and appeared effective for lung-targeted anti-inflammatory action.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
