

Intersection of biology and therapeutics: type 2 targeted therapeutics for adult asthma
- PMID: 32007172
- PMCID: PMC8522504
- DOI: 10.1016/S0140-6736(19)33005-3
Intersection of biology and therapeutics: type 2 targeted therapeutics for adult asthma
Abstract
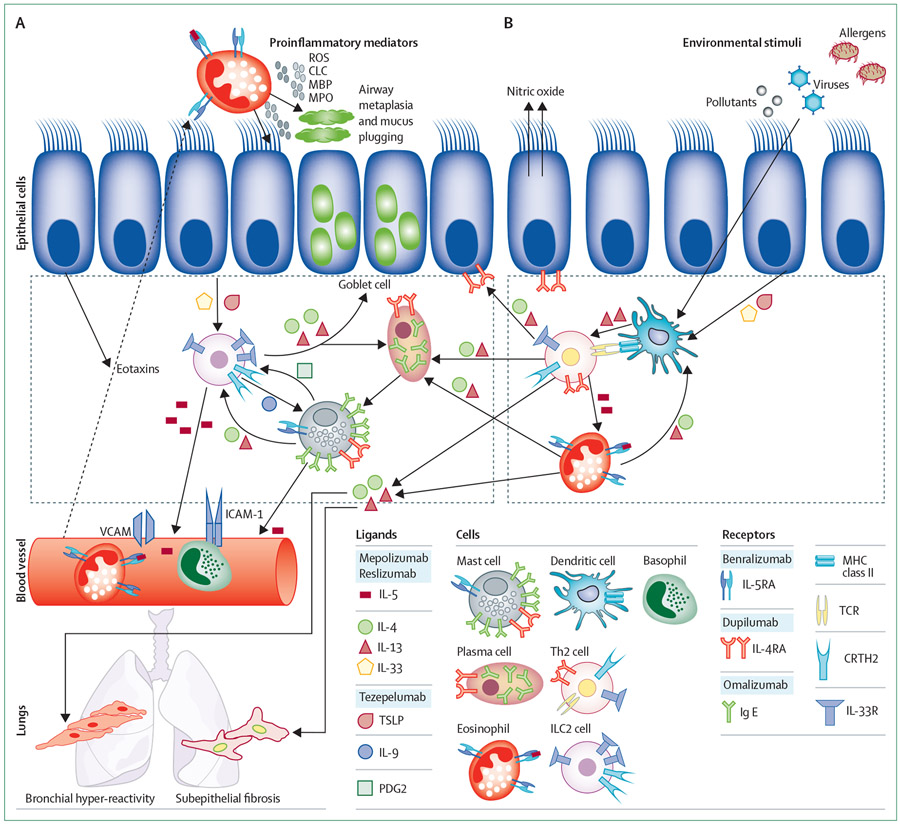
Asthma is a disease of reversible airflow obstruction characterised clinically by wheezing, shortness of breath, and coughing. Increases in airway type 2 cytokine activity, including interleukin-4 (IL-4), IL-5, and IL-13, are now established biological mechanisms in asthma. Inhaled corticosteroids have been the foundation for asthma treatment, in a large part because they decrease airway type 2 inflammation. However, inhaled or systemic corticosteroids are ineffective treatments in many patients with asthma and few treatment options exist for patients with steroid resistant asthma. Although mechanisms for corticosteroid refractory asthma are likely to be numerous, the development of a new class of biologic agents that target airway type 2 inflammation has provided a new model for treating some patients with corticosteroid refractory asthma. The objective of this Therapeutic paper is to summarise the new type 2 therapeutics, with an emphasis on the biological rationale and clinical efficacy of this new class of asthma therapeutics.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
MCP reports personal fees from Merck, and grants from AstraZeneca, Boehringer Ingelheim, Genentech, GlaxoSmithKline (GSK), Sanofi Genzyme-Regeneron, and TEVA Pharmaceuticals Industries, outside the submitted work. SEW reports grants and personal fees from Sanofi, AstraZeneca, GSK, grants from Novartis, and personal fees from Pieris Pharmaceuticals. She also reports grants from AstraZeneca, Boehringer-Ingelheim, Genentech, GSK, Sanofi Genzyme-Regeneron, and Teva Pharmaceuticals Industries, outside the submitted work.
Figures

References
-
- Wenzel SE. Complex phenotypes in asthma: current definitions. Pulm Pharmacol Ther 2013; 26: 710–15. - PubMed
-
- Aaron SD, Vandemheen KL, FitzGerald JM, et al. Reevaluation of diagnosis in adults with physician-diagnosed asthma. JAMA 2017; 317: 269–79. - PubMed
-
- Pavord ID, Beasley R, Agusti A, et al. After asthma: redefining airways diseases. Lancet 2018; 391: 350–400. - PubMed
-
- Anderson GP. Endotyping asthma: new insights into key pathogenic mechanisms in a complex, heterogeneous disease. Lancet 2008; 372: 1107–19. - PubMed
