

Socioeconomic Status and Sleep among Couples
- PMID: 32008377
- PMCID: PMC7395863
- DOI: 10.1080/15402002.2020.1721501
Socioeconomic Status and Sleep among Couples
Abstract
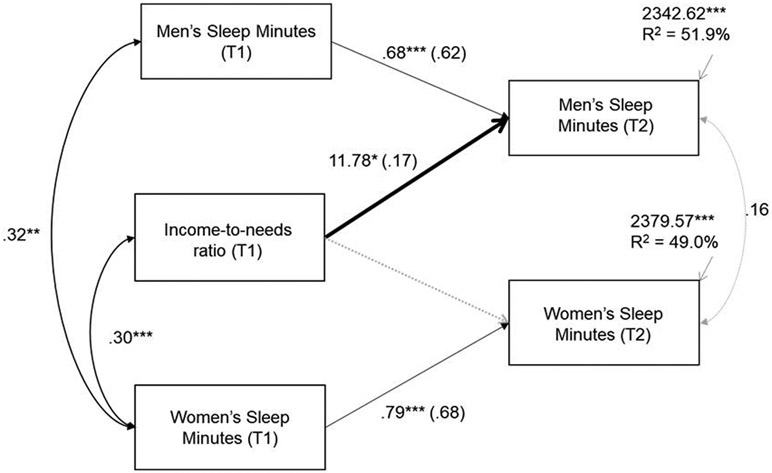
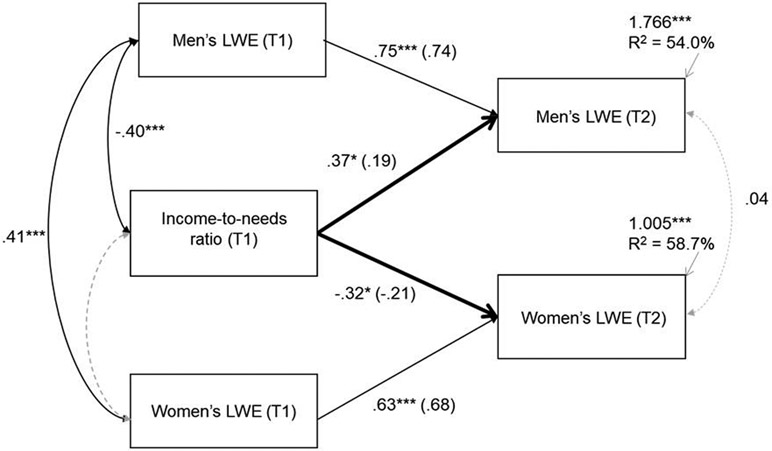
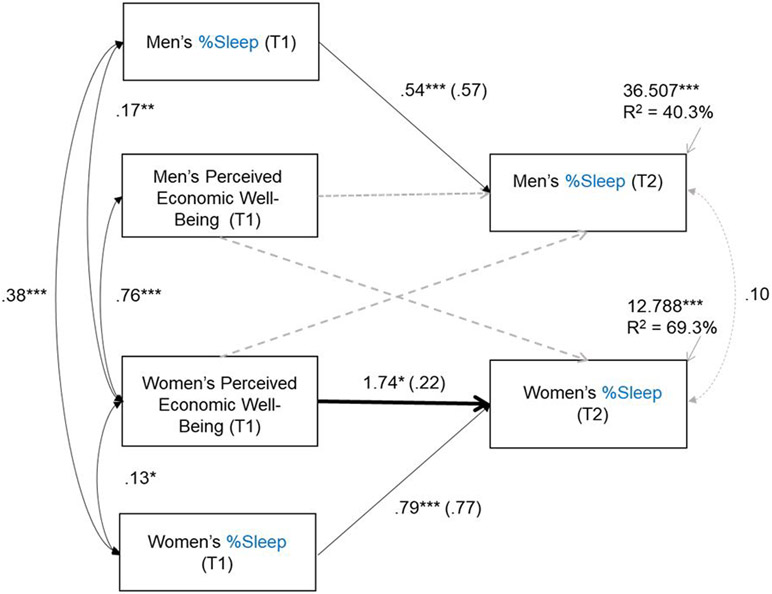
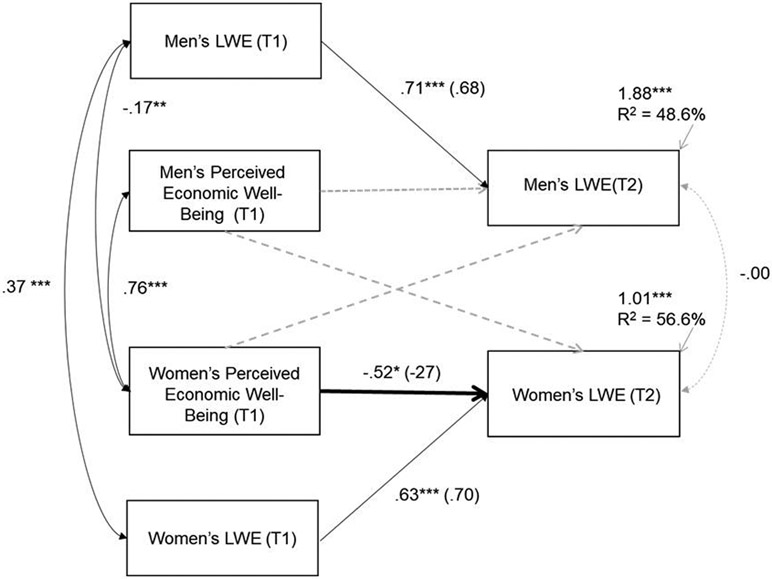
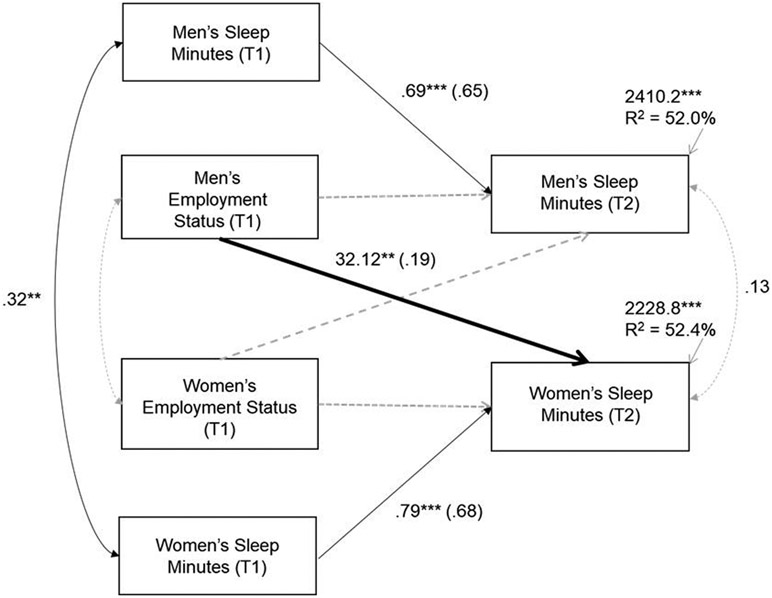
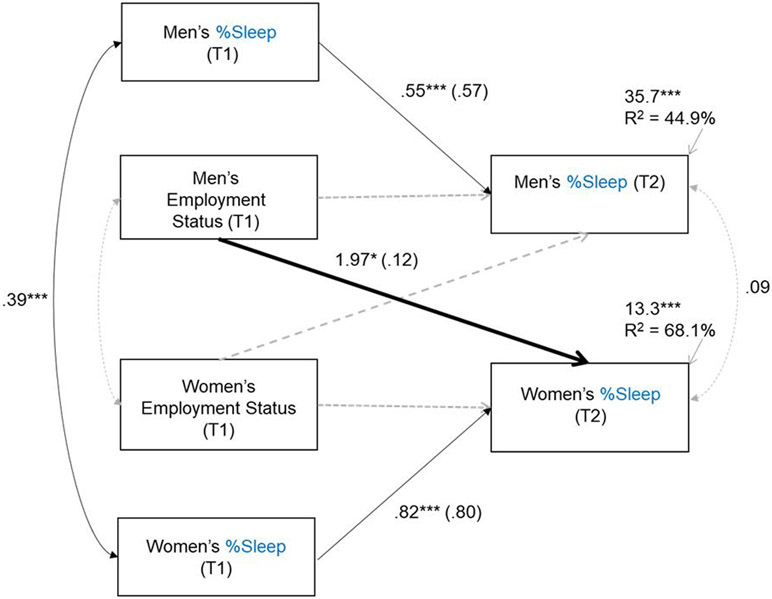
Objective/Background: Lower socioeconomic status (SES) is generally associated with poor sleep but little is known about how different SES indices are associated with sleep duration and quality, or about these relations longitudinally or in cohabiting couples. The main objective was to examine longitudinal associations between multiple SES and sleep parameters in cohabiting adults. Participants: Participants were cohabiting couples (N = 135) of women (M age = 37.2 years, SD = 5.93; 76% White/European American, 18% Black/African American) and men (M = 39.9 years, SD = 7.33; 78% White, 18% Black). Methods: Men and women participated twice with a 1-year lag. At Time (T1), participants reported on multiple SES indices including their income, perceived economic well-being, education, employment status, and occupation. Sleep at T1 and T2 was assessed with self-reports and actigraphs (sleep duration from onset to wake time, %sleep from onset to wake, long wake episodes). Results: Actor effects on actigraphy-assessed sleep parameters were evident for both men and women; low SES was associated with shorter duration and poor quality (%sleep, long wake episodes) sleep. These associations were most pronounced for income-to-needs ratio (men and women) and perceived economic well-being (women only). Partner effects were also evident such that men's employment status was associated with women's longer sleep duration and greater sleep quality (%sleep) whereas women's employment predicted increased subjective sleep problems for men. Conclusion: Findings illustrate the need to consider multiple SES and sleep indices, as well as the family context in studies addressing linkages between SES and sleep.
Figures

References
-
- Acebo C, & Carskadon MA (2001). Scoring actigraph data using ACTION-W 2. Providence, RI: Bradley Sleep Center, Brown University.
-
- Acock AC (2005). Working with missing values. Journal of Marriage and Family, 67(4), 1012–1028. doi:10.1111/j.1741-3737.2005.00191.x - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical