

Unsupervised Machine Learning Reveals Novel Traumatic Brain Injury Patient Phenotypes with Distinct Acute Injury Profiles and Long-Term Outcomes
- PMID: 32008422
- PMCID: PMC7249479
- DOI: 10.1089/neu.2019.6705
Unsupervised Machine Learning Reveals Novel Traumatic Brain Injury Patient Phenotypes with Distinct Acute Injury Profiles and Long-Term Outcomes
Abstract
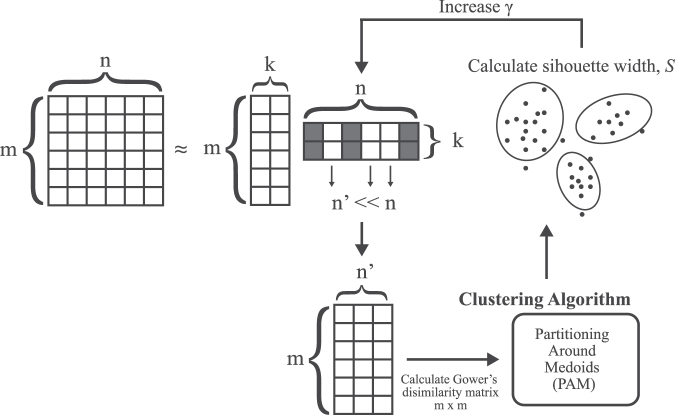
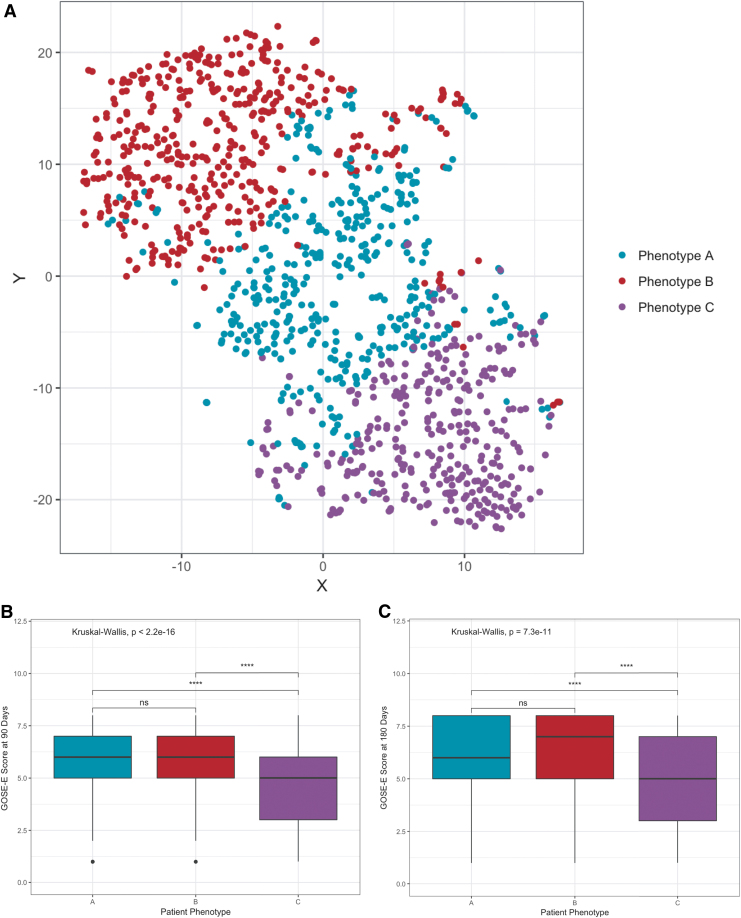
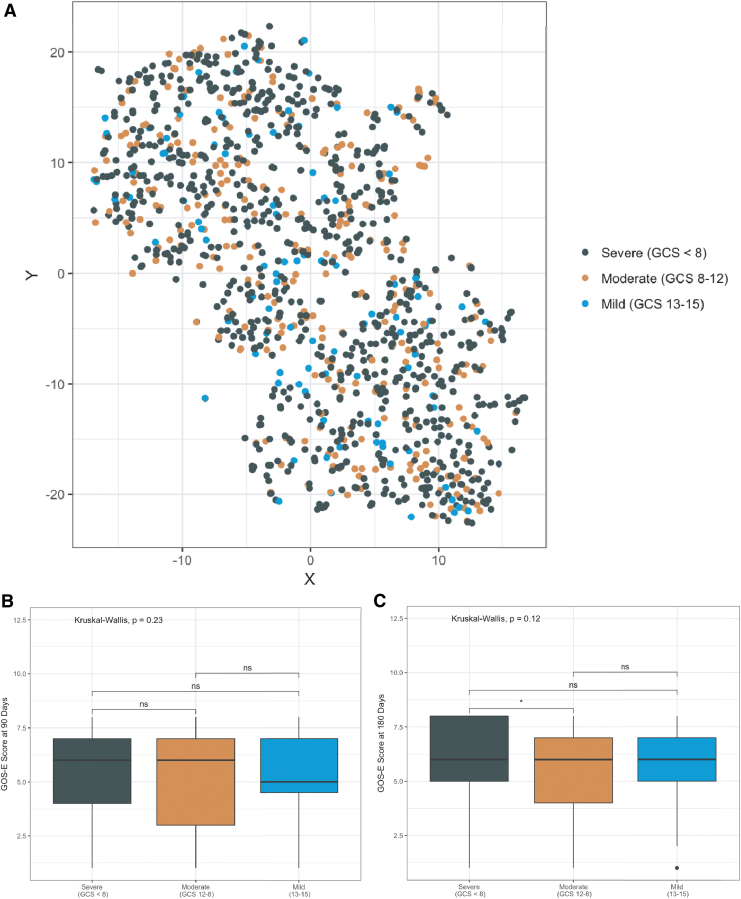
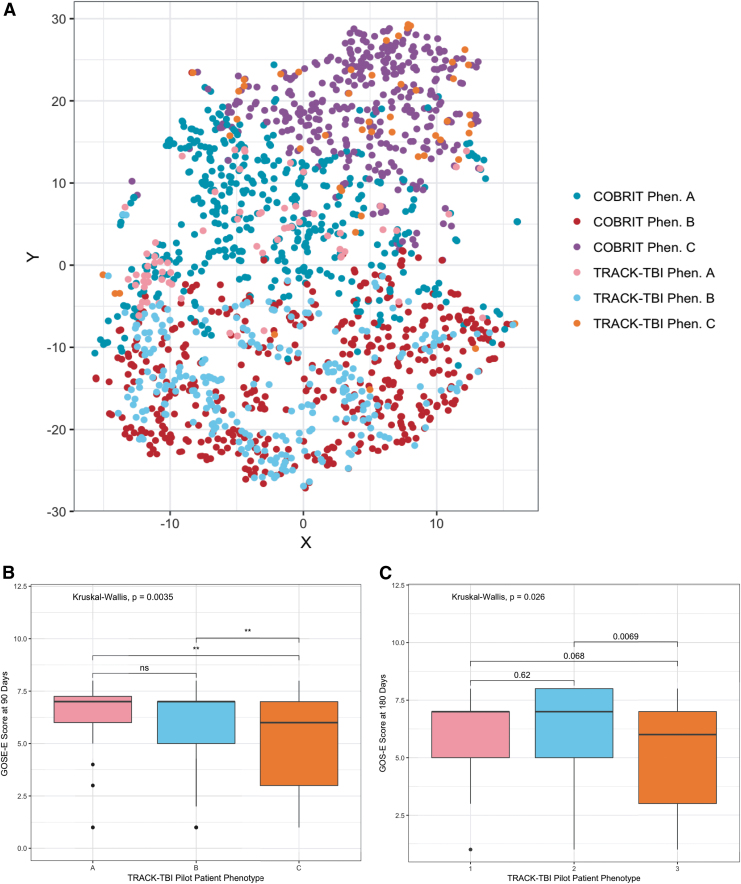
The heterogeneity of traumatic brain injury (TBI) remains a core challenge for the success of interventional clinical trials. Data-driven approaches for patient stratification may help to identify TBI patient phenotypes during the acute injury period as well as facilitate targeted trial patient enrollment and analysis of treatment efficacy. In this study, we implemented an unsupervised machine learning approach to identify TBI subpopulations at injury baseline using data from 1213 TBI patients who participated in the Citicoline Brain Injury Treatment Trial (COBRIT) Trial. A wrapper framework utilizing generalized low-rank models automatically selected relevant clinical features that were subsequently used to cluster patients using a partitioning around medoids clustering algorithm. Using this approach, we identified three patient phenotypes with unique clinical injury profiles based on a subset of acute injury features. Phenotype-specific differences in long-term functional outcome trajectories were respectively observed at 3 and 6 months after injury. In comparison, when patients were grouped by baseline Glasgow Coma Scale (GCS), no differences in baseline clinical feature profiles or long-term outcomes were observed. To test phenotype reproducibility in an external validation data set, we used a K-nearest neighbors algorithm to classify subjects in the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) Pilot data set into corresponding phenotypes, then measured the Gower's dissimilarities between TRACK-TBI and COBRIT subjects in each phenotype. No significant differences were found between trial subjects within two phenotypes, suggesting that these phenotypes may be generalizable within a broad range of TBI severity. Further, Extended Glasgow Outcome Scale (GOS-E) outcomes in the TRACK-TBI data set similarly demonstrated phenotype-specific differences in long-term outcomes. Our results suggest that unsupervised machine learning is a promising and effective approach for discovery of novel injury subpopulations over the conventional GCS-based method, and may improve patient selection in future TBI clinical trials.
Keywords: GCS; TBI; clinical trial; machine learning; unsupervised clustering.
Conflict of interest statement
No competing financial interests exist.
Figures
Comment in
-
Data-driven approaches to reveal the pathobiological heterogeneity in patients with traumatic brain injury.Intensive Care Med. 2023 Sep;49(9):1107-1109. doi: 10.1007/s00134-023-07156-y. Epub 2023 Jul 20. Intensive Care Med. 2023. PMID: 37470833 Free PMC article. No abstract available.
-
Response to Folweiler KA et al., Unsupervised Machine Learning Reveals Novel Traumatic Brain Injury Patient Phenotypes With Distinct Acute Injury Profiles and Long-Term Outcomes (DOI: 10.1089/neu.2019.6705).J Neurotrauma. 2024 Jan;41(1-2):292-293. doi: 10.1089/neu.2023.0396. Epub 2023 Oct 18. J Neurotrauma. 2024. PMID: 37756375 No abstract available.
-
Response to Wang et al., Unsupervised machine learning reveals novel traumatic brain injury patient phenotypes with distinct acute injury profiles and long-term outcomes (doi: 10.1089/neu.2019.6705).J Neurotrauma. 2024 Feb;41(3-4):539. doi: 10.1089/neu.2023.0478. Epub 2023 Dec 20. J Neurotrauma. 2024. PMID: 37776180 No abstract available.
References
-
- Maas A.I.R., Steyerberg E.W., Murray G.D., Bullock R., Baethmann A., Marshall L.F., and Teasdale G.M. (1999). Why have recent trials of neuroprotective agents in head injury failed to show convincing efficacy? A pragmatic analysis and theoretical considerations. Neurosurgery 44, 1286–1298 - PubMed
-
- Narayan R.K., Michel M.E., Ansell B., Baethmann A., Biegon A., Bracken M.B., Bullock M.R., Choi S.C., Clifton G.L., Contant C.F., Coplin W.M., Dietrich W.D., Ghajar J., Grady S.M., Grossman R.G., Hall E.D., Heetderks W., Hovda D.A., Jallo J., Katz R.L., Knoller N., Kochanek P.M., Maas A.I., Majde J., Marion D.W., Marmarou A., Marshall L.F., McIntosh T.K., Miller E., Mohberg N., Muizelaar J.P., Pitts L.H., Quinn P., Riesenfeld G., Robertson C.S., Strauss K.I., Teasdale G., Temkin N., Tuma R., Wade C., Walker M.D., Weinrich M., Whyte J., Wilberger J., Young A.B., and Yurkewicz L. (2002). Clinical trials in head injury. J. Neurotrauma 19, 503–557 - PMC - PubMed
-
- Marshall L.F. (2000). Head injury: recent past, present, and future. Neurosurgery 47, 546–61 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
