

Real-world behavior of CRT pacing using the AdaptivCRT algorithm on patient outcomes: Effect on mortality and atrial fibrillation incidence
- PMID: 32009263
- PMCID: PMC7187461
- DOI: 10.1111/jce.14376
Real-world behavior of CRT pacing using the AdaptivCRT algorithm on patient outcomes: Effect on mortality and atrial fibrillation incidence
Abstract
Background: The AdaptivCRT (aCRT) algorithm continuously adjusts cardiac resynchronization therapy (CRT) according to intrinsic atrioventricular conduction, providing synchronized left ventricular pacing in patients with normal PR interval and adaptive BiV pacing in patients with prolonged PR interval. Previous analyses demonstrated an association between aCRT and clinical benefit. We evaluated the incidence of patient mortality and atrial fibrillation (AF) with aCRT compared with standard CRT in a real-world population.
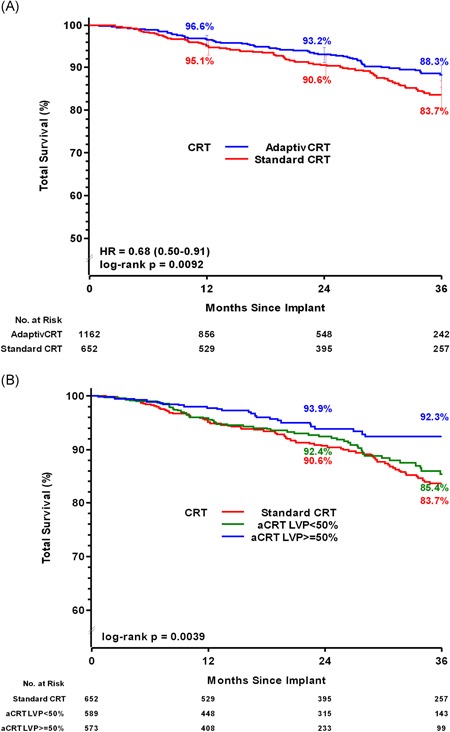
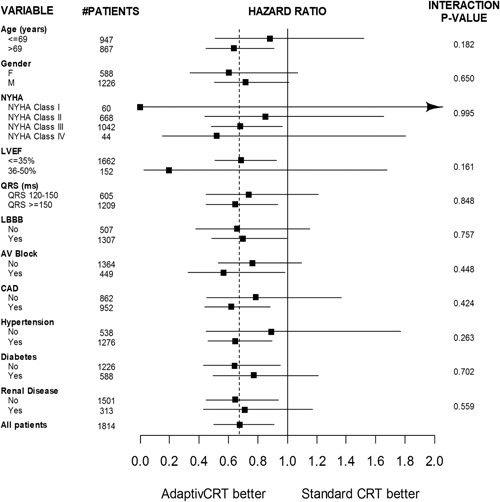
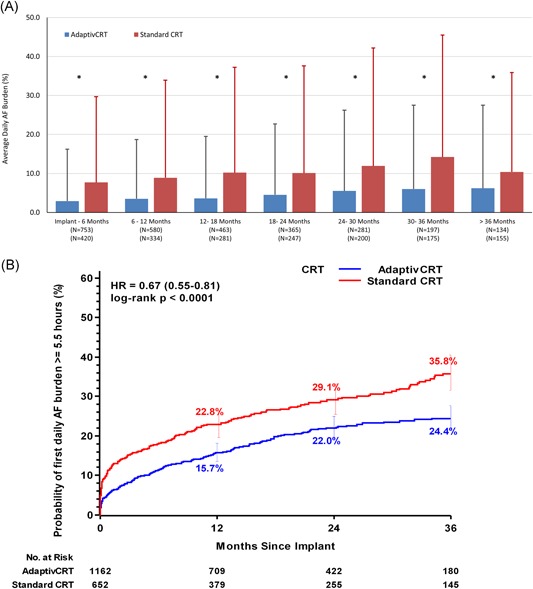
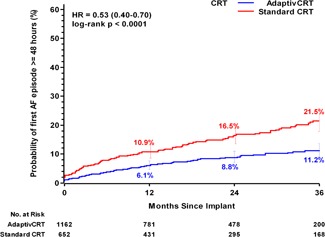
Methods and results: Patients enrolled in the Medtronic Personalized CRT Registry and implanted with a CRT from 2013-2018 were divided into aCRT ON or standard CRT groups based upon device-stored data. A Frailty survival model was used to evaluate the potential survival benefit of aCRT, accounting for patient heterogeneity and center variability. Daily AF burden and first device-detected AF episodes of various durations were recorded by the device during follow-up. A total of 1814 CRT patients with no reported long-standing AF history at implant were included. Mean follow-up time was 26.1 ± 16.5 months and 1162 patients (64.1%) had aCRT ON. Patient survival probability at 36 months was 88.3% for aCRT ON and 83.7% for standard CRT (covariate-adjusted hazard ratio [HR] = 0.71, 95% CI: 0.53-0.96, P = .028). Mean AF burden during follow-up was consistently lower in aCRT ON patients compared with standard CRT. At 36 months, the probability of AF was lower in patients with aCRT ON, regardless of which AF definition threshold was applied (6 minutes-30 days, all P < .001).
Conclusion: Use of the AdaptivCRT algorithm was associated with improved patient survival and lower incidence of AF in a real-world, prospective, nonrandomized registry.
Trial registration: ClinicalTrials.gov NCT01524276.
Keywords: AV conduction; atrial fibrillation; cardiac resynchronization therapy; heart failure; optimized pacing; synchronized pacing.
© 2020 The Authors. Journal of Cardiovascular Electrophysiology Published by Wiley Periodicals, Inc.
Figures
References
-
- Brignole M, Auricchio A, Baron‐Esquivias G, et al. ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013;34:2281‐2329. - PubMed
-
- Zipes DP, Camm AJ, Borggrefe M, et al. American College of Cardiology/American Heart Association Task Force, European Society of Cardiology Committee for Practice Guidelines, European Heart Rhythm Association, Heart Rhythm Society: ACC/AHA/ESC 2006 Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention Of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114:e385‐e484. - PubMed
-
- Linde C, Abraham WT, Gold MR, et al. Predictors of short‐term clinical response to cardiac resynchronization therapy. Eur J Heart Fail. 2017;19:1056‐1063. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
