

Safety and Utility of Cardiopulmonary Exercise Testing in Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia
- PMID: 32009524
- PMCID: PMC7033873
- DOI: 10.1161/JAHA.119.013695
Safety and Utility of Cardiopulmonary Exercise Testing in Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia
Abstract
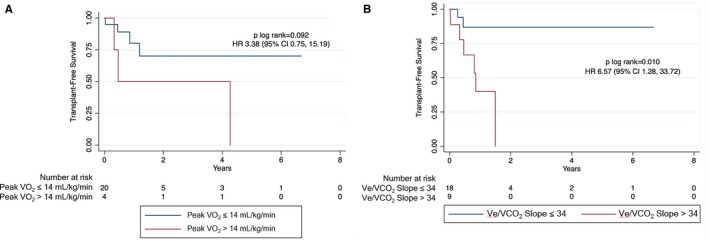
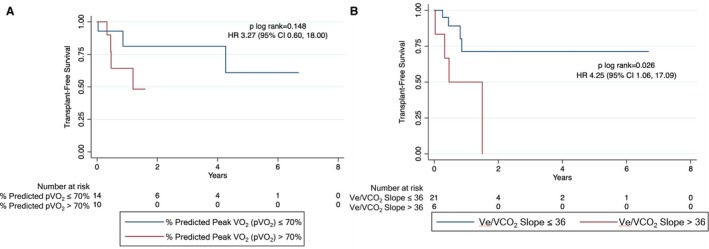
Background Arrhythmogenic right ventricular cardiomyopathy/dysplasia (ARVC/D) is characterized by high arrhythmic burden and progressive heart failure, which can prompt referral for heart transplantation. Cardiopulmonary exercise testing (CPET) has an established role in risk stratification for advanced heart failure therapies, but has not been described in ARVC/D. This study sought to determine the safety and prognostic utility of CPET in patients with ARVC/D. Methods and Results Using the Johns Hopkins ARVC/D Registry, we examined patients with ARVC/D undergoing CPET. Baseline characteristics and transplant-free survival were compared on the basis of peak oxygen consumption (pVO2) (≤14 or >14 mL/kg per minute) and ventilatory efficiency (Ve/VCO2 slope ≤34 or >34). Thirty-eight patients underwent 50 CPETs. There were no sustained arrhythmic events. Twenty-nine patients achieved a maximal test. Patients with pVO2 ≤14 mL/kg per minute were more often men (P=0.042) compared with patients with pVO2 >14 mL/kg per minute. Patients with Ve/VCO2 slope >34 tended to have more moderate/severe right ventricular dilation (7/9 [78%] versus 10/26 [38%]; P=0.060) and clinical heart failure (8/9 [89%] versus 13/26 [50%]; P=0.056) compared with patients with Ve/VCO2 slope ≤34. Patients who underwent heart transplantation were more likely to have clinical heart failure (10/10 [100%] versus 13/28 [46%]; P=0.003). Patients with Ve/VCO2 slope >34 had worse transplant-free survival compared with patients with Ve/VCO2 slope ≤34 (n=35; hazard ratio, 6.57 [95% CI, 1.28-33.72]; log-rank P=0.010), whereas transplant-free survival was similar on the basis of pVO2 groups (n=29; hazard ratio, 3.38 [95% CI, 0.75-15.19]; log-rank P=0.092). Conclusions CPET is safe to perform in patients with ARVC/D. Ve/VCO2 slope may be used for risk stratification and guide referral for heart transplantation in ARVC/D.
Keywords: arrhythmias; cardiomyopathy; exercise testing; genetics; heart failure; transplantation.
Figures
Comment in
-
Predicting Heart Failure in Arrhythmogenic Right Ventricular Cardiomyopathy.J Am Heart Assoc. 2020 Feb 4;9(3):e015702. doi: 10.1161/JAHA.119.015702. Epub 2020 Feb 3. J Am Heart Assoc. 2020. PMID: 32009530 Free PMC article. No abstract available.
References
-
- Calkins H. Arrhythmogenic right ventricular dysplasia/cardiomyopathy. Circ J. 2015;79:901–913. - PubMed
-
- Dalal D, Nasir K, Bomma C, Prakasa K, Tandri H, Piccini J, Roguin A, Tichnell C, James C, Russell SD, Judge DP, Abraham T, Spevak PJ, Bluemke DA, Calkins H. Arrhythmogenic right ventricular dysplasia: a United States experience. Circulation. 2005;112:3823–3832. - PubMed
-
- Gandjbakhch E, Redheuil A, Pousset F, Charron P, Frank R. Clinical diagnosis, imaging, and genetics of arrhythmogenic right ventricular cardiomyopathy/dysplasia. J Am Coll Cardiol. 2018;72:784–804. - PubMed
-
- Gilotra NA, Bhonsale A, James CA, te Riele ASJ, Murray B, Tichnell C, Swant A, Ong CS, Judge DPJ, Russell SD, Calkins H, Tedford RJ. Heart failure is common and under‐recognized in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia. Circ Heart Fail. 2017;10:1–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
