

Moderate Hypothermia Modifies Coronary Hemodynamics and Endothelium-Dependent Vasodilation in a Porcine Model of Temperature Management
- PMID: 32009525
- PMCID: PMC7033898
- DOI: 10.1161/JAHA.119.014035
Moderate Hypothermia Modifies Coronary Hemodynamics and Endothelium-Dependent Vasodilation in a Porcine Model of Temperature Management
Abstract
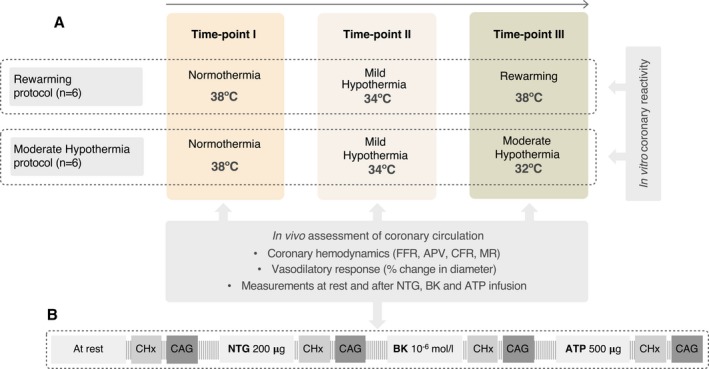
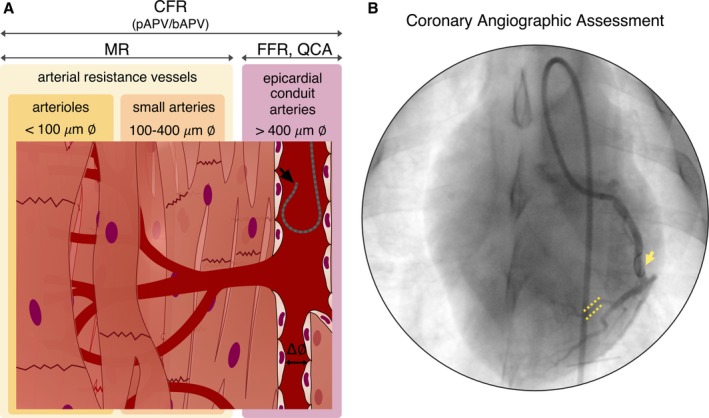
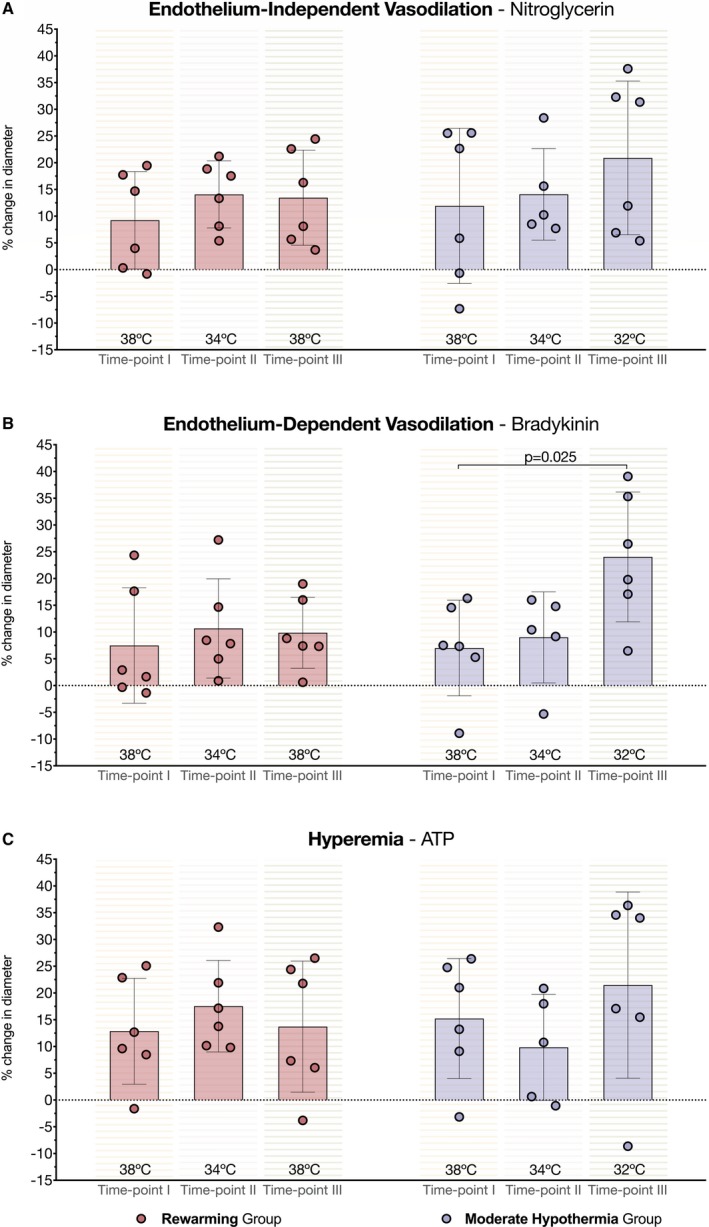
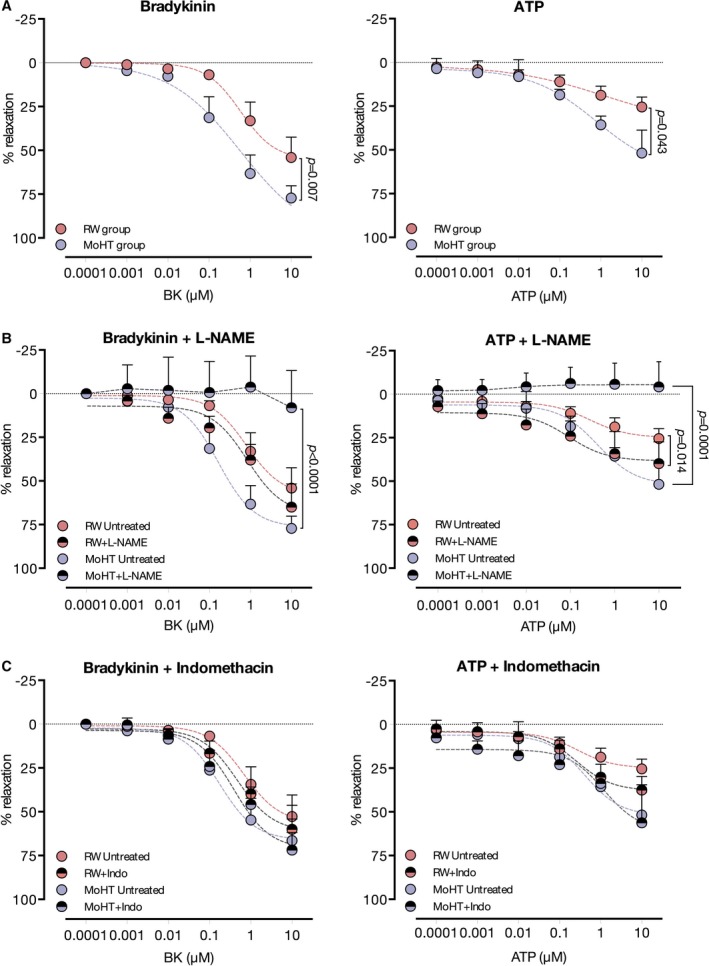
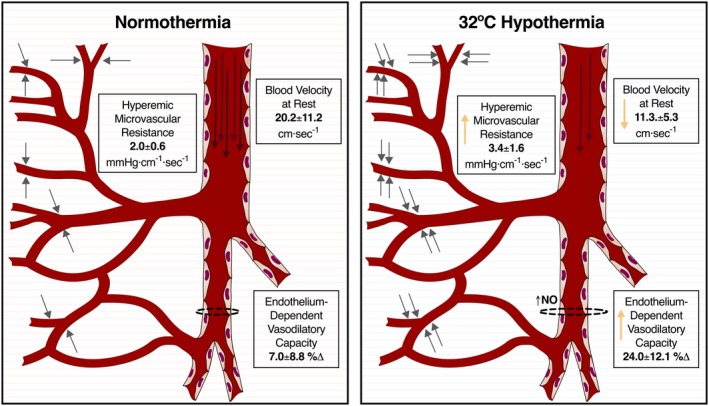
Background Hypothermia has been associated with therapeutic benefits including reduced mortality and better neurologic outcomes in survivors of cardiac arrest. However, undesirable side effects have been reported in patients undergoing coronary interventions. Using a large animal model of temperature management, we aimed to describe how temperature interferes with the coronary vasculature. Methods and Results Coronary hemodynamics and endothelial function were studied in 12 pigs at various core temperatures. Left circumflex coronary artery was challenged with intracoronary nitroglycerin, bradykinin, and adenosine at normothermia (38°C) and mild hypothermia (34°C), followed by either rewarming (38°C; n=6) or moderate hypothermia (MoHT; 32°C, n=6). Invasive coronary hemodynamics by Doppler wire revealed a slower coronary blood velocity at 32°C in the MoHT protocol (normothermia 20.2±11.2 cm/s versus mild hypothermia 18.7±4.3 cm/s versus MoHT 11.3±5.3 cm/s, P=0.007). MoHT time point was also associated with high values of hyperemic microvascular resistance (>3 mm Hg/cm per second) (normothermia 2.0±0.6 mm Hg/cm per second versus mild hypothermia 2.0±0.8 mm Hg/cm per second versus MoHT 3.4±1.6 mm Hg/cm per second, P=0.273). Assessment of coronary vasodilation by quantitative coronary analysis showed increased endothelium-dependent (bradykinin) vasodilation at 32°C when compared with normothermia (normothermia 6.96% change versus mild hypothermia 9.01% change versus MoHT 25.42% change, P=0.044). Results from coronary reactivity in vitro were in agreement with angiography data and established that endothelium-dependent relaxation in MoHT completely relies on NO production. Conclusions In this porcine model of temperature management, 34°C hypothermia and rewarming (38°C) did not affect coronary hemodynamics or endothelial function. However, 32°C hypothermia altered coronary vasculature physiology by slowing coronary blood flow, increasing microvascular resistance, and exacerbating endothelium-dependent vasodilatory response.
Keywords: NO; coronary physiology; endothelium; microcirculation; therapeutic hypothermia.
Figures
References
-
- Alzaga AG, Cerdan M, Varon J. Therapeutic hypothermia. Resuscitation. 2006;70:369–380. - PubMed
-
- HACA Study Group . Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out‐of‐hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
