

Hypogonadism and Cryptorchidism
- PMID: 32010061
- PMCID: PMC6974459
- DOI: 10.3389/fendo.2019.00906
Hypogonadism and Cryptorchidism
Abstract
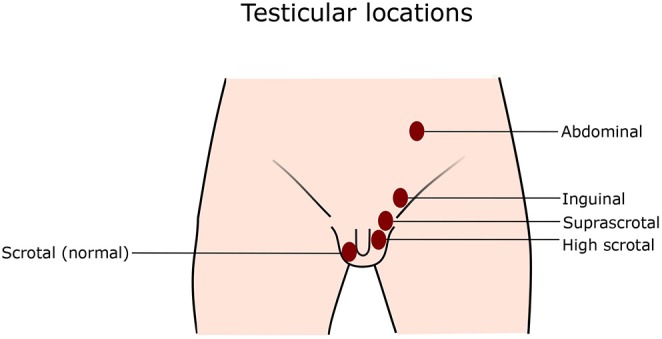
Congenital cryptorchidism (undescended testis) is one of the most common congenital urogenital malformations in boys. Prevalence of cryptorchidism at birth among boys born with normal birth weight ranges from 1.8 to 8.4%. Cryptorchidism is associated with a risk of low semen quality and an increased risk of testicular germ cell tumors. Testicular hormones, androgens and insulin-like peptide 3 (INSL3), have an essential role in the process of testicular descent from intra-abdominal position into the scrotum in fetal life. This explains the increased prevalence of cryptorchidism among boys with diseases or syndromes associated with congenitally decreased secretion or action of androgens, such as patients with congenital hypogonadism and partial androgen insensitivity syndrome. There is evidence to support that cryptorchidism is associated with decreased testicular hormone production later in life. It has been shown that cryptorchidism impairs long-term Sertoli cell function, but may also affect Leydig cells. Germ cell loss taking place in the cryptorchid testis is proportional to the duration of the condition, and therefore early orchiopexy to bring the testis into the scrotum is the standard treatment. However, the evidence for benefits of early orchiopexy for testicular endocrine function is controversial. The hormonal treatments using human chorionic gonadotropin (hCG) or gonadotropin-releasing hormone (GnRH) to induce testicular descent have low success rates, and therefore they are not recommended by the current guidelines for management of cryptorchidism. However, more research is needed to assess the effects of hormonal treatments during infancy on future male reproductive health.
Keywords: Leydig cell; Sertoli cell; gonadotropins; testosterone; undescended testis.
Copyright © 2020 Rodprasert, Virtanen, Mäkelä and Toppari.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources