

Immunohistochemical Expression of Epidermal Growth Factor Receptor in Astrocytic Tumors in Iraqi Patients
- PMID: 32010368
- PMCID: PMC6986536
- DOI: 10.3889/oamjms.2019.751
Immunohistochemical Expression of Epidermal Growth Factor Receptor in Astrocytic Tumors in Iraqi Patients
Abstract
Background: Diffuse astrocytomas constitute the largest group of primary malignant human intracranial tumours. They are classified by the World Health Organization (WHO) into three histological malignancy grades: diffuse astrocytomas (grade II), anaplastic astrocytomas (grade III) and glioblastoma (grade IV) based on histopathological features such as cellular atypia, mitotic activity, necrosis and microvascular proliferation. Epidermal growth factor receptor (EGFR) is a 170-kDa transmembrane tyrosine kinase receptor expressed in a variety of normal and malignant cells regulating critical cellular processes. When activated, epidermal growth factor receptor (EGFR) triggers several signalling cascades leading to increased proliferation and angiogenesis and decreased apoptosis and hence associated with aggressive progression of the tumour. Epidermal growth factor receptor (EGFR) level is known to be a strong indicator associated with the aggressive behaviour of the tumour and acts as a prognostic factor for evaluating the survival rate.
Aim: To evaluate the expression of epidermal growth factor receptor (EGFR) in different grades of astrocytoma.
Material and methods: formalin-fixed paraffin-embedded astrocytic tumours of 44 patients were collected from the archival material of pathology department of Ghazi Al Hariri Teaching Hospital during the period from June to December 2018. Hematoxylin and eosin-stained sections were used to characterise the tumours histologically based on cellularity, nuclear hyperchromasia, polymorphism, mitotic activity, vascular proliferation and necrosis with or without pseudopallisading of tumour cells. Diagnosis and grading of astrocytic tumours in this study were made according to WHO criteria (2016). Using a monoclonal antibody to the epidermal growth factor receptor (EGFR) and immunohistochemical analysis, the expression and distribution of epidermal growth factor receptor in astrocytic tumours were examined.
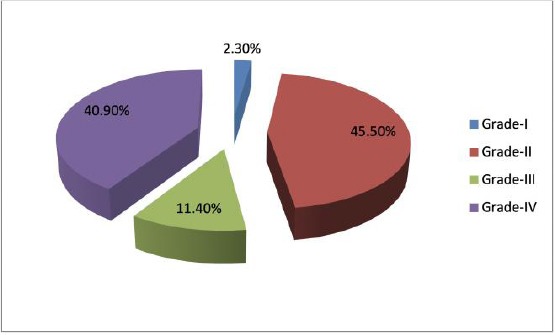
Results: The study included 1 case pilocytic astrocytoma (grade I), 20 cases diffuse astrocytoma (grade II), 5 cases anaplastic astrocytoma (grade III) and 18 cases of glioblastoma (grade IV). Expression of EGFR was found in 38.88% of the glioblastoma samples (grade IV). However, none of the astrocytomas of WHO grades I, II and III showed immunoreactivity for EGFR protein. Different patterns of immunoreactive cells and significant intratumor heterogeneity of EGFR expression were observed in glioblastomas.
Conclusion: The immunohistochemical expression of Epidermal growth factor receptor (EGFR) was restricted only to high-grade astrocytic tumours, namely glioblastoma, thus may use to predict glioblastoma.
Keywords: Astrocytoma; Epidermal growth factor receptor; Glioblastoma.
Copyright: © 2019 Mohanad Mundher Abdulghani, Mohamad Natiq Abbas, Wafaa Redha Mohammed.
Figures


References
-
- Lacy J, Saadati H, Yu J. Complications of brain tumors and their treatment. Hemat Oncol Clin North Am. 2012;26(4):779–796. https://doi.org/10.1016/j.hoc.2012.04.007 PMid:22794283. - PubMed
-
- Jacques G, Cormac O. Central nervous system tumors. Handb Clin Neurol. 2013;112:931–958. https://doi.org/10.1016/B978-0-444-52910-7.00015-5 PMid:23622303. - PubMed
-
- Counsell C, Grant R. Incidence studies of primary and secondary intracranial tumors:a systematic review of their methodology and results. J Neurooncol. 1998;37(3):241–250. https://doi.org/10.1023/A:1005861024679 PMid:9524082. - PubMed
-
- Ostrom QT, Gittleman H, Truitt G, et al. CBTRUS Statistical Report:Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011-2015. Neuro Oncol. 2018;20(4):iv1. https://doi.org/10.1093/neuonc/noy131 PMid:30445539 PMCid:PMC6129949. - PMC - PubMed
-
- Kohler BA, Ward E, McCarthy BJ, et al. Annual report to the nation on the status of cancer 1975-2007, featuring tumors of the brain and other nervous system. J Natl Cancer Inst. 2011;103:714. https://doi.org/10.1093/jnci/djr077 PMid:21454908 PMCid:PMC3086878. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous