

Pharmacokinetics and Pharmacodynamics of Anti-infective Agents during Continuous Veno-venous Hemofiltration in Critically Ill Patients: Lessons Learned from an Ancillary Study of the IVOIRE Trial
- PMID: 32010602
- PMCID: PMC6985915
- DOI: 10.2478/jtim-2019-0031
Pharmacokinetics and Pharmacodynamics of Anti-infective Agents during Continuous Veno-venous Hemofiltration in Critically Ill Patients: Lessons Learned from an Ancillary Study of the IVOIRE Trial
Abstract
Background: Hemofiltration rate, changes in blood and ultrafiltration flow, and discrepancies between the prescribed and administered doses strongly influence pharmacokinetics (PK) and pharmacodynamics (PD) of antimicrobial agents during continuous veno-venous hemofiltration (CVVH) in critically ill patients.
Methods: Ancillary data were from the prospective multicenter IVOIRE (hIgh VOlume in Intensive caRE) study. High volume (HV, 70 mL/kg/h) was at random compared with standard volume (SV, 35 mL/kg/h) CVVH in septic shock patients with acute kidney injury (AKI). PK/PD parameters for all antimicrobial agents used in each patient were studied during five days.
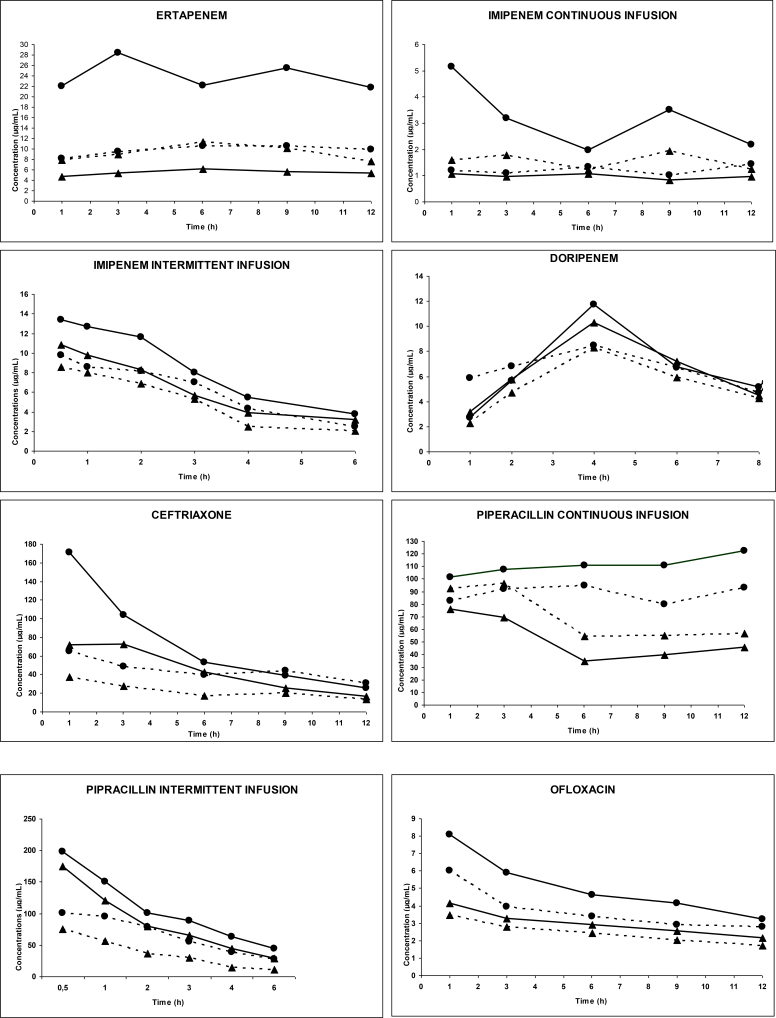
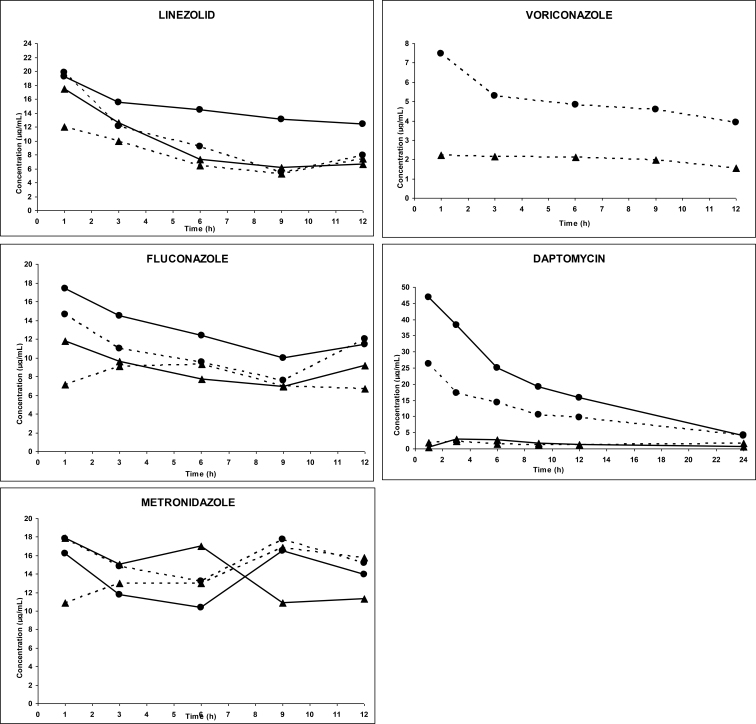
Results: Antimicrobial treatment met efficacy targets for both percentage of time above the minimal inhibitory concentration and inhibitory quotient. A significant correlation was observed between the ultrafiltration flow and total systemic clearance (Spearman test: P < 0.005) and between CVVH clearance and drug elimination half-life (Spearman test: P < 0.005). All agents were easily filtered. Mean sieving coefficient ranged from 38.7% to 96.7%. Mean elimination half-life of all agents was significantly shorter during HV-CVVH (from 1.29 to 28.54 h) than during SV-CVVH (from 1.51 to 33.85 h) (P < 0.05).
Conclusions: This study confirms that CVVH influences the PK/PD behavior of most antimicrobial agents. Antimicrobial elimination was directly correlated with convection rate. Current antimicrobial dose recommendations will expose patients to underdosing and increase the risk for treatment failure and development of resistance. Dose recommendations are proposed for some major antibiotic and antifungal treatments in patients receiving at least 25 mL/kg/h CVVH.
Keywords: antibiotic dosage; antibiotics; continuous veno-venous hemofiltration; high volume hemofiltration; pharmacodynamics; pharmacokinetics; septic shock.
© 2019 Dominique Breilh et al., published by Sciendo.
Conflict of interest statement
Conflict of Interest The authors declare to have no competing interests.
Figures
References
-
- Roberts JA, Lipman J. Pharmacokinetic issues for antibiotics in the critically ill patient. Crit Care Med. 2009;37:840–51. quiz 859. - PubMed
-
- Bugge JF. Pharmacokinetics and drug dosing adjustments during continuous venovenous hemofiltration or hemodiafiltration in critically ill patients. Acta Anaesthesiol Scand. 2001;45:929–34. - PubMed
-
- Trotman RL, Williamson JC, Shoemaker DM, Salzer WL. Antibiotic dosing in critically ill adult patients receiving continuous renal replacement therapy. Clin Infect Dis. 2005;41:1159–66. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous