

Guidelines for Diuretic Utilization Reduce High Charge Medications
- PMID: 32010863
- PMCID: PMC6946231
- DOI: 10.1097/pq9.0000000000000237
Guidelines for Diuretic Utilization Reduce High Charge Medications
Abstract
Decreasing practice variation and following evidence-based clinical guidelines improve patient outcomes and often reduce cost. Essentially all postsurgical cardiac patients require diuretics. The approach to diuresis in the pediatric cardiothoracic intensive care unit (CTICU) is not standardized. Our objective was to develop and implement guidelines for diuretic utilization in the CTICU to reduce high charge medication utilization while maintaining the delivery of high-quality care.
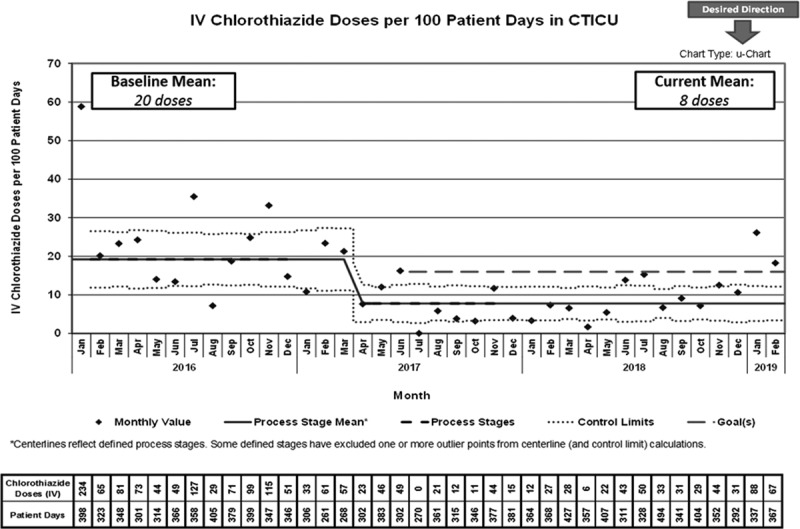
Methods: Two of the top 10 medications by charge in the CTICU during 2016 were diuretics [fenoldopam and intravenous (IV) chlorothiazide]. Standardized diuretic utilization guidelines were developed to reduce the utilization of fenoldopam and IV chlorothiazide. We implemented guidelines in April 2017. The utilization of fenoldopam and IV chlorothiazide, as well as overall diuretic charges, before and after guideline implementation were compared.
Results: We normalized all comparisons to 100 CTICU patient-days. Fenoldopam starts were reduced from 1.1 in 2016 to 0.03 in 2019 (through February); days of fenoldopam use were reduced from 4 in 2016 to 0.15 days in 2019 (through February); IV chlorothiazide doses decreased from 20 in 2016 to 8 in 2019 (through February). These changes reduced the mean charges for diuretics from $25,762 in 2016 to $8,855 in 2019 (through February). CTICU average daily census did not change significantly during the study period (12.8 in 2016 vs 11.8 in 2018).
Conclusion: Value-added implementation of standardized diuretic utilization guidelines in the CTICU successfully reduced the use of high-charge diuretics without unfavorably impacting the quality of care delivery.
Copyright © 2019 the Author(s). Published by Wolters Kluwer Health, Inc.
Figures





References
-
- McCammond AN, Axelrod DM, Bailly DK, et al. Pediatric cardiac intensive care society 2014 consensus statement: pharmacotherapies in cardiac critical care fluid management. Pediatr Crit Care Med. 2016;17(3 Suppl 1):S35–S48. - PubMed
-
- Hirleman E, Larson DF. Cardiopulmonary bypass and edema: physiology and pathophysiology. Perfusion. 2008;23:311–322. - PubMed
-
- Wolfer RS, Bishop GG, Burdett MG, et al. Extravascular fluid uptake during cardiopulmonary bypass in hypertensive dogs. Ann Thorac Surg. 1994;57:974–980. - PubMed
-
- Wernovsky G, Wypij D, Jonas RA, et al. Postoperative course and hemodynamic profile after the arterial switch operation in neonates and infants. A comparison of low-flow cardiopulmonary bypass and circulatory arrest. Circulation. 1995;92:2226–2235. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous