

Endoscopic Resection of Ampullary Tumours: Long-term Outcomes and Adverse Events
- PMID: 32010876
- PMCID: PMC6985700
- DOI: 10.1093/jcag/gwz007
Endoscopic Resection of Ampullary Tumours: Long-term Outcomes and Adverse Events
Abstract
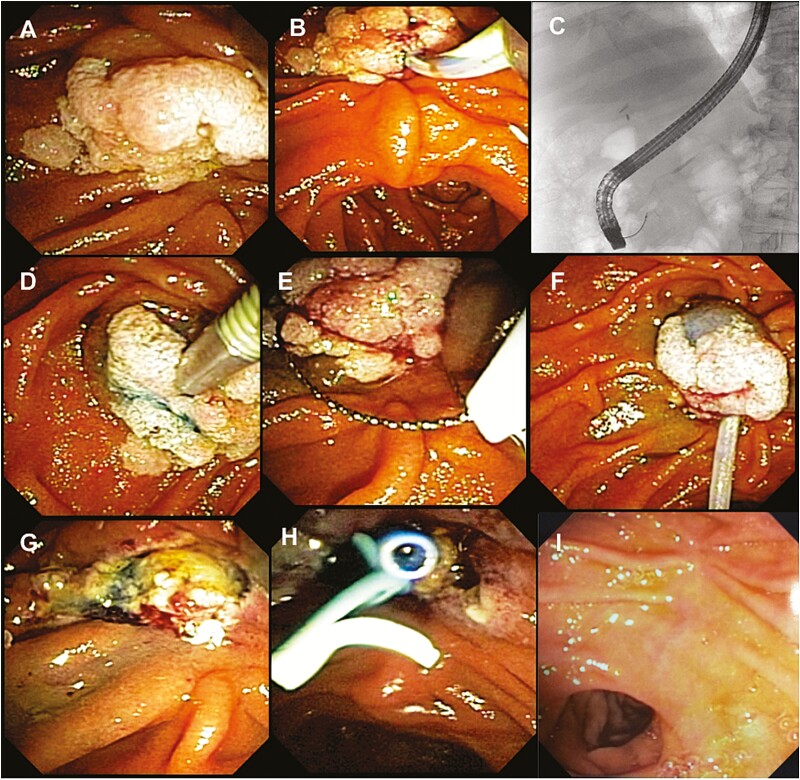
Background: The management of ampullary lesions has shifted from surgical approach to endoscopic resection. Previous reports were limited by small numbers of patients and short follow-up. The aim of this study is to describe short- and long-term outcomes in a large cohort of patients undergoing endoscopic ampullectomy.
Methods: Retrospective study of endoscopic ampullectomies performed at a tertiary center from January 1999 to October 2016. Information recorded includes patient demographics, clinical outcomes, lesion pathology, procedural events, adverse events and follow-up data.
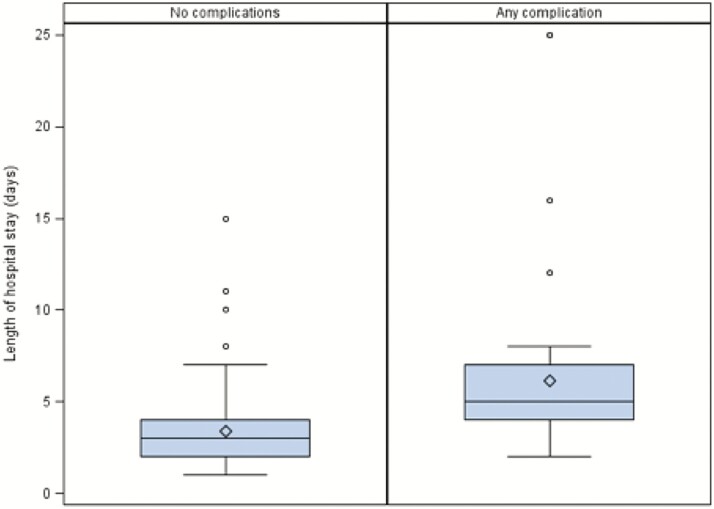
Results: Overall, 103 patients underwent endoscopic resection of ampullary tumours (mean age 62.3 ± 14.3 years, 50.5% female, mean lesion size 20.9 mm; 94.9% adenomas, with a majority of lesions exhibiting low-grade dysplasia (72.7%). Complete endoscopic resection was achieved in 82.5% at initial procedure. Final complete endoscopic resection was achieved in all patients with benign pathology on follow-up procedures. Final pathology showed that 11% had previously undiagnosed invasive carcinoma. Delayed postprocedure bleeding occurred in 21.4%, all of which were managed successfully at endoscopy. Acute pancreatitis complicated 15.5% of procedures (mild in 93.8%). Perforation occurred in 5.8%, all treated conservatively except for one patient requiring surgery. Piecemeal resection was associated with significantly higher recurrence compared to en-bloc resection (54.3% versus 26.2%, respectively, P = 0.012). All recurrences were treated endoscopically.
Conclusion: Endoscopic ampullectomy appears both safe and effective in managing patients with ampullary tumours in experienced hands. Most adverse events can be managed conservatively. Many patients develop recurrence during long-term follow-up but can be managed endoscopically. Recurrence rates may be reduced by performing initial en-bloc resection.
Keywords: Adenoma; Ampulla; Ampullectomy; ERCP; Polypectomy.
© The Author(s) 2019. Published by Oxford University Press on behalf of the Canadian Association of Gastroenterology.
Figures
References
-
- Han J, Kim MH. Endoscopic papillectomy for adenomas of the major duodenal papilla (with video). Gastrointest Endosc 2006;63(2):292–301. - PubMed
-
- Kim HK, Lo SK. Endoscopic approach to the patient with benign or malignant ampullary lesions. Gastrointest Endosc Clin N Am 2013;23(2):347–83. - PubMed
-
- El Hajj II, Coté GA. Endoscopic diagnosis and management of ampullary lesions. Gastrointest Endosc Clin N Am 2013;23(1):95–109. - PubMed
-
- Rosenberg J, Welch JP, Pyrtek LJ, et al. Benign villous adenomas of the ampulla of Vater. Cancer 1986;58(7):1563–8. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials