

Performance of cardiopulmonary exercise testing for the prediction of post-operative complications in non cardiopulmonary surgery: A systematic review
- PMID: 32012165
- PMCID: PMC6996804
- DOI: 10.1371/journal.pone.0226480
Performance of cardiopulmonary exercise testing for the prediction of post-operative complications in non cardiopulmonary surgery: A systematic review
Abstract
Introduction: Cardiopulmonary exercise testing (CPET) is widely used within the United Kingdom for preoperative risk stratification. Despite this, CPET's performance in predicting adverse events has not been systematically evaluated within the framework of classifier performance.
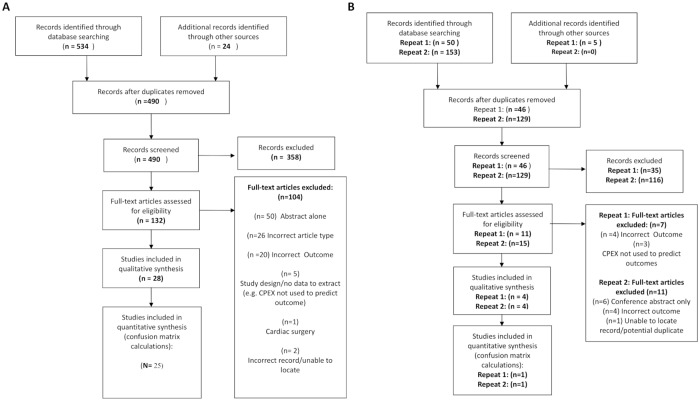
Methods: After prospective registration on PROSPERO (CRD42018095508) we systematically identified studies where CPET was used to aid in the prognostication of mortality, cardiorespiratory complications, and unplanned intensive care unit (ICU) admission in individuals undergoing non-cardiopulmonary surgery. For all included studies we extracted or calculated measures of predictive performance whilst identifying and critiquing predictive models encompassing CPET derived variables.
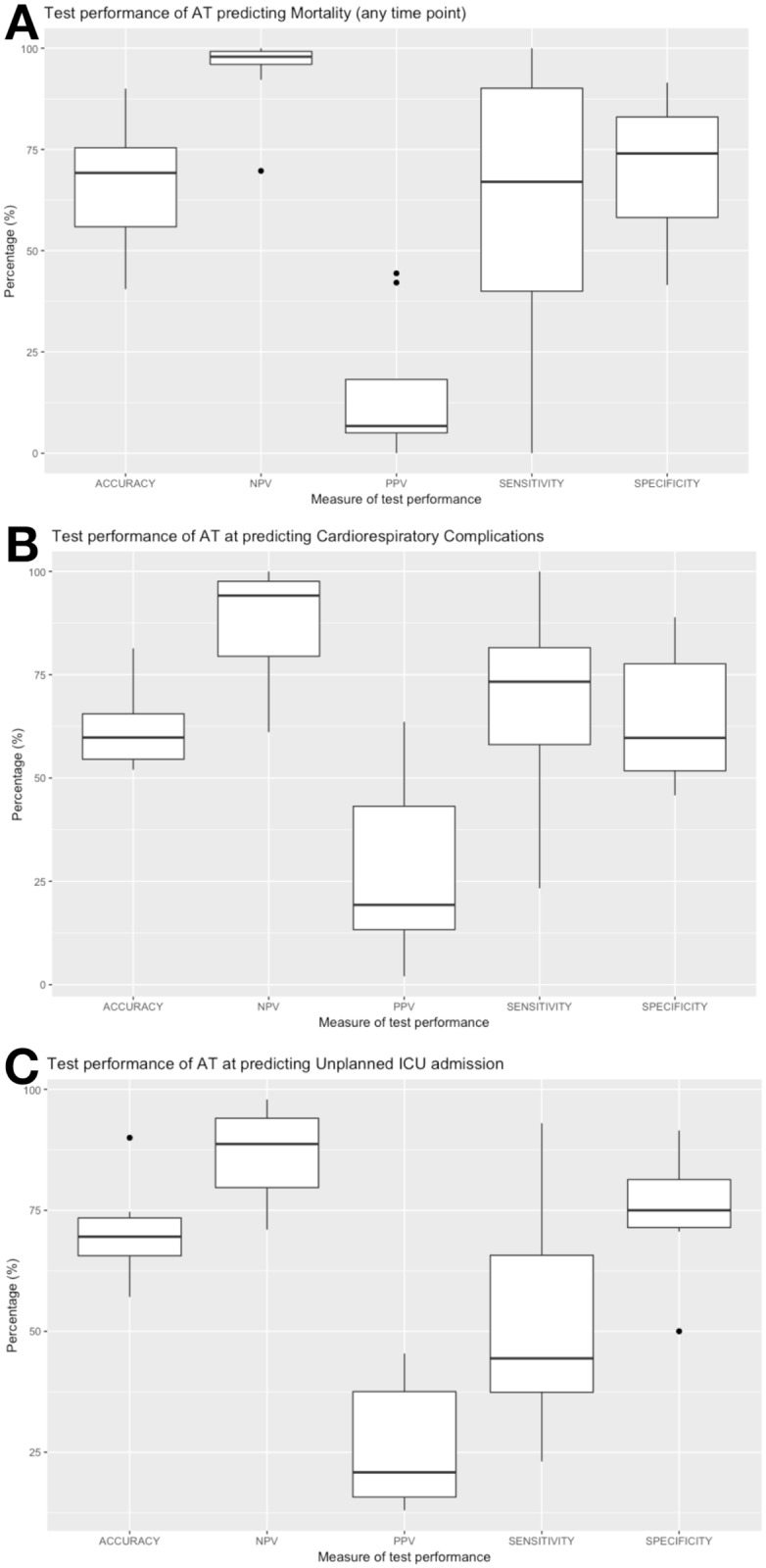
Results: We identified 36 studies for qualitative review, from 27 of which measures of classifier performance could be calculated. We found studies to be highly heterogeneous in methodology and quality with high potential for bias and confounding. We found seven studies that presented risk prediction models for outcomes of interest. Of these, only four studies outlined a clear process of model development; assessment of discrimination and calibration were performed in only two and only one study undertook internal validation. No scores were externally validated. Systematically identified and calculated measures of test performance for CPET demonstrated mixed performance. Data was most complete for anaerobic threshold (AT) based predictions: calculated sensitivities ranged from 20-100% when used for predicting risk of mortality with high negative predictive values (96-100%). In contrast, positive predictive value (PPV) was poor (2.9-42.1%). PPV appeared to be generally higher for cardiorespiratory complications, with similar sensitivities. Similar patterns were seen for the association of Peak VO2 (sensitivity 85.7-100%, PPV 2.7-5.9%) and VE/VCO2 (Sensitivity 27.8%-100%, PPV 3.4-7.1%) with mortality.
Conclusions: In general CPET's 'rule-out' capability appears better than its ability to 'rule-in' complications. Poor PPV may reflect the frequency of complications in studied populations. Our calculated estimates of classifier performance suggest the need for a balanced interpretation of the pros and cons of CPET guided pre-operative risk stratification.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- NELA Project Team The fourth patient report of the National Emergency Laparotomy Audit. RCoA London, 2018. Available at: https://www.nela.org.uk/reports.
-
- Agnew N Preoperative cardiopulmonary exercise testing Contin Educ Anaesthesia, Crit Care Pain. 2010; 10: 33–37.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
