

Characterizing Hepatitis C Virus-Specific CD4+ T Cells Following Viral-Vectored Vaccination, Directly Acting Antivirals, and Spontaneous Viral Cure
- PMID: 32012325
- PMCID: PMC7610807
- DOI: 10.1002/hep.31160
Characterizing Hepatitis C Virus-Specific CD4+ T Cells Following Viral-Vectored Vaccination, Directly Acting Antivirals, and Spontaneous Viral Cure
Abstract
Background and aims: Induction of functional helper CD4+ T cells is the hallmark of a protective immune response against hepatitis C virus (HCV), associated with spontaneous viral clearance. Heterologous prime/boost viral vectored vaccination has demonstrated induction of broad and polyfunctional HCV-specific CD8+ T cells in healthy volunteers; however, much less is known about CD4+ T-cell subsets following vaccination.
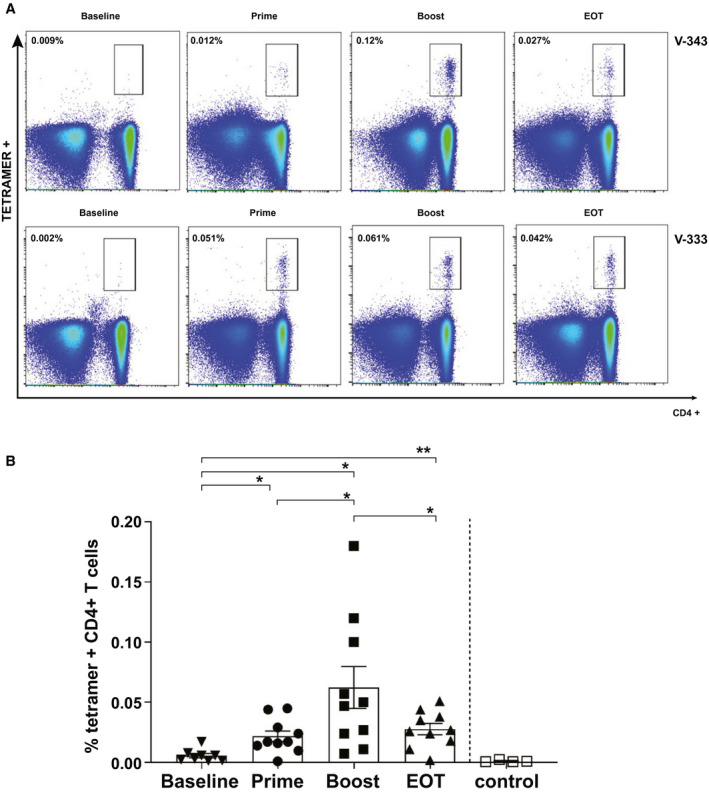
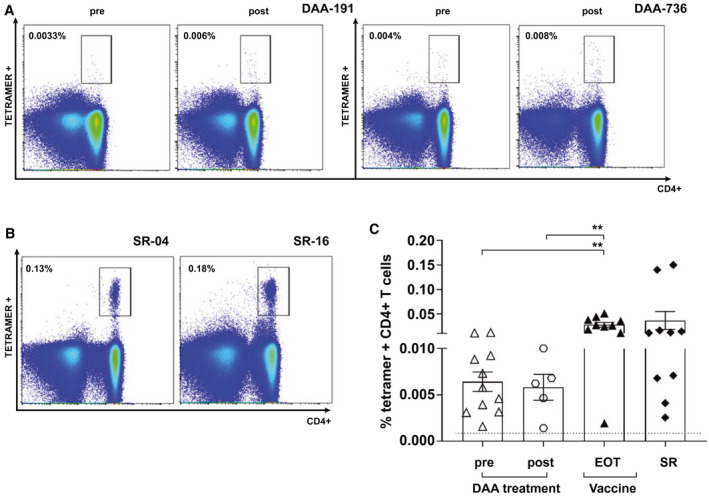
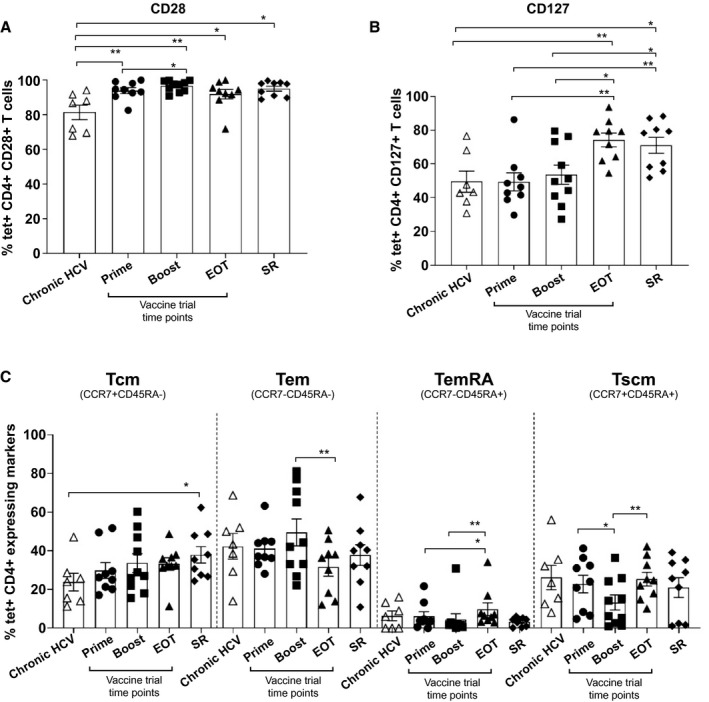
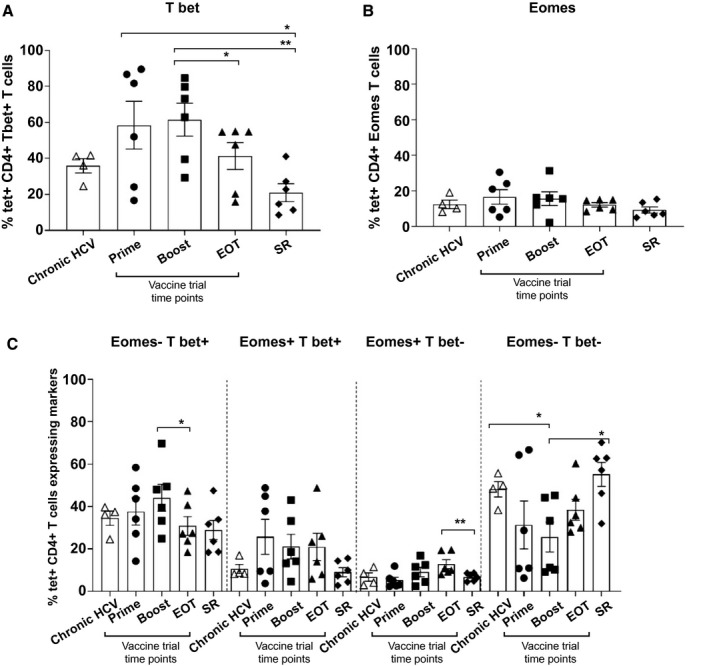
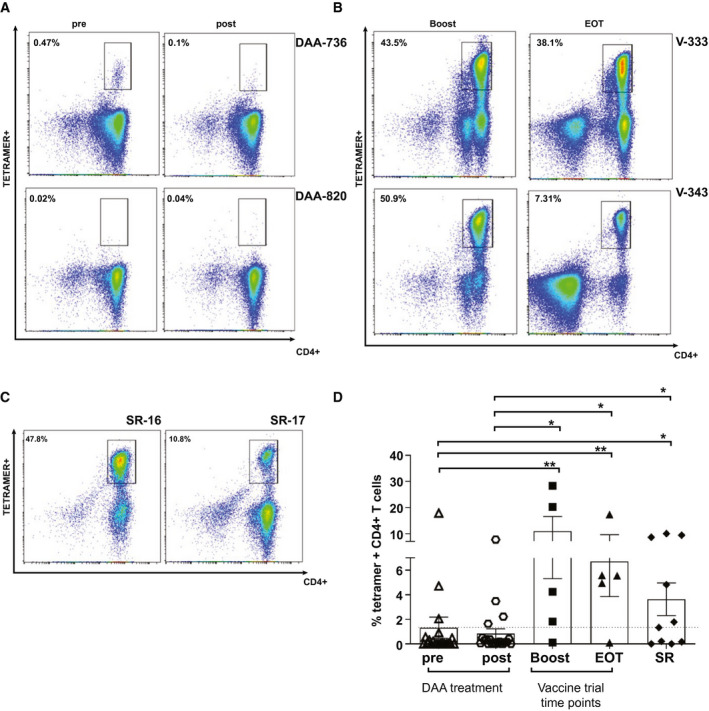
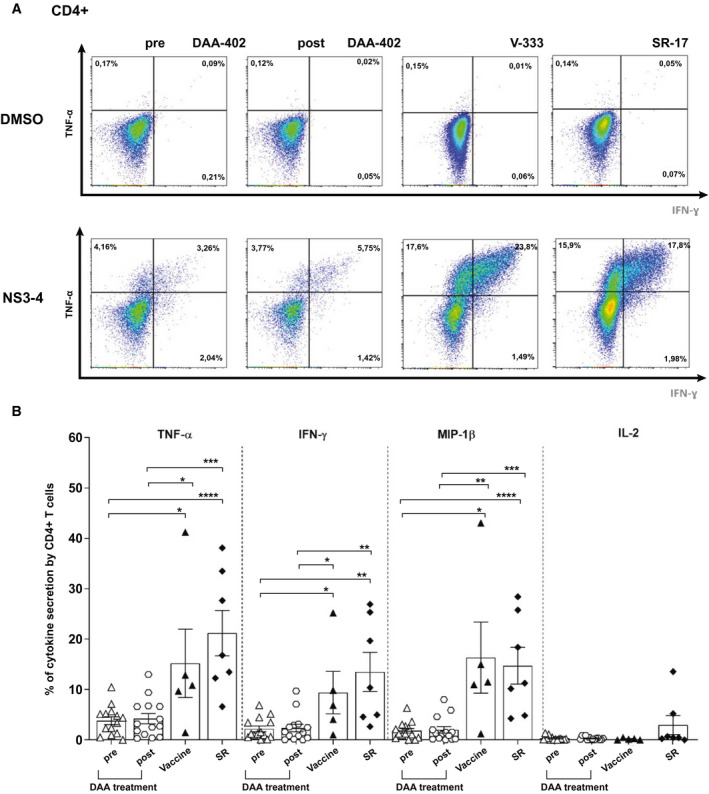
Approach and results: We analyzed HCV-specific CD4+ T-cell populations using major histocompatibility complex class II tetramers in volunteers undergoing HCV vaccination with recombinant HCV adenoviral/modified vaccinia Ankara viral vectors. Peptide-specific T-cell responses were tracked over time, and functional (proliferation and cytokine secretion) and phenotypic (cell surface and intranuclear) markers were assessed using flow cytometry. These were compared to CD4+ responses in 10 human leukocyte antigen-matched persons with HCV spontaneous resolution and 21 chronically infected patients treated with directly acting antiviral (DAA) therapy. Vaccination induced tetramer-positive CD4+ T cells that were highest 1-4 weeks after boosting (mean, 0.06%). Similar frequencies were obtained for those tracked following spontaneous resolution of disease (mean, 0.04%). In addition, the cell-surface phenotype (CD28, CD127) memory subset markers and intranuclear transcription factors, as well as functional capacity of peptide-specific CD4+ T-cell responses characterized after vaccination, are comparable to those following spontaneous viral resolution. In contrast, helper responses in chronic infection were infrequently detected and poorly functional and did not consistently recover following HCV cure.
Conclusions: Helper CD4+ T-cell phenotype and function following HCV viral vectored vaccination resembles "protective memory" that is observed following spontaneous clearance of HCV. DAA cure does not promote resurrection of exhausted CD4+ T-cell memory in chronic infection.
© 2020 by the American Association for the Study of Liver Diseases.
Figures
References
-
- WHO . Global Hepatitis Report, 2017. Geneva, Switzerland: WHO; 2017:1‐83.
-
- Lauer GM, Walker BD. Hepatitis C virus infection. N Engl J Med 2001;345:41‐52. - PubMed
-
- Grakoui A, Shoukry NH, Woollard DJ, Han JH, Hanson HL, Ghrayeb J, et al. HCV persistence and immune evasion in the absence of memory T cell help. Science 2003;302:659‐662. - PubMed
-
- Diepolder HM, Zachoval R, Hoffmann RM, Jung MC, Pape GR, Wierenga EA, et al. Possible mechanism involving T‐lymphocyte response to non‐structural protein 3 in viral clearance in acute hepatitis C virus infection. Lancet 1995;346:1006‐1007. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
