

Shoulder Muscle Strength and Neuromuscular Activation 2 Years after Reverse Shoulder Prosthesis-An Experimental Case Control Study
- PMID: 32013074
- PMCID: PMC7073832
- DOI: 10.3390/jcm9020365
Shoulder Muscle Strength and Neuromuscular Activation 2 Years after Reverse Shoulder Prosthesis-An Experimental Case Control Study
Abstract
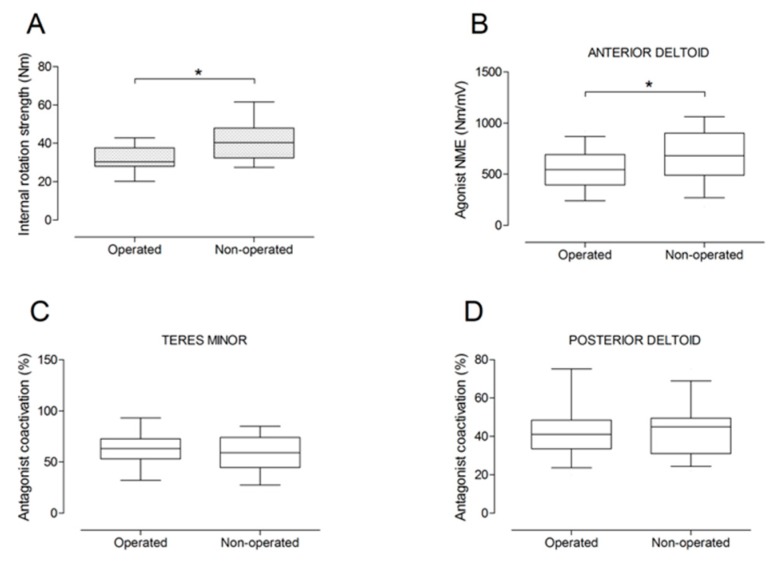
Although reverse shoulder arthroplasty (RSA) has shown successful postoperative outcomes, little is known about compensatory activation patterns of remaining shoulder muscles following RSA. The purpose of this experimental case control series was to investigate shoulder muscle strength and neuromuscular activation of deltoid and teres minor muscles 2 years after RSA. Humerus lengthening, center-of-rotation medialization, maximal voluntary strength, and electromyographic (EMG) activity were compared between the operated and the non-operated side of 13 patients (mean age: 73 years). Shoulder muscle strength was significantly lower on the operated side for external rotation (-54%), internal rotation (-20%), and adduction (-13%). Agonist deltoid EMG activity was lower on the operated side for shoulder flexion, extension, and internal and external rotation (p < 0.05). Antagonist deltoid coactivation was higher on the operated side for external rotation (p < 0.001). Large correlation coefficients were observed between shoulder adductor strength asymmetry and both center-of-rotation medialization (r = -0.73) and humerus lengthening (r = 0.71). Shoulder abduction strength and neuromuscular activation were well preserved 2 years after RSA, while persistent strength and activation deficits were observed for shoulder adduction and internal and external rotation. Additional studies are required to elucidate shoulder neuromuscular activation patterns before and after RSA to support decision making for surgical, implant design, and rehabilitation choices.
Keywords: deltoid muscle; electromyography; humerus lengthening; muscle strength; neuromuscular activation; reverse shoulder arthroplasty.
Conflict of interest statement
The authors declare no conflict of interest.
Figures









References
-
- Jobin C.M., Brown G.D., Bahu M.J., Gardner T.R., Bigliani L.U., Levine W.N., Ahmad C.S. Reverse total shoulder arthroplasty for cuff tear arthropathy: the clinical effect of deltoid lengthening and center of rotation medialization. J. Shoulder Elbow Surg. 2012;21:1269–1277. doi: 10.1016/j.jse.2011.08.049. - DOI - PubMed
LinkOut - more resources
Full Text Sources
