

Vitamin C Intravenous Treatment In the Setting of Atrial Fibrillation Ablation: Results From the Randomized, Double-Blinded, Placebo-Controlled CITRIS-AF Pilot Study
- PMID: 32013700
- PMCID: PMC7033876
- DOI: 10.1161/JAHA.119.014213
Vitamin C Intravenous Treatment In the Setting of Atrial Fibrillation Ablation: Results From the Randomized, Double-Blinded, Placebo-Controlled CITRIS-AF Pilot Study
Abstract
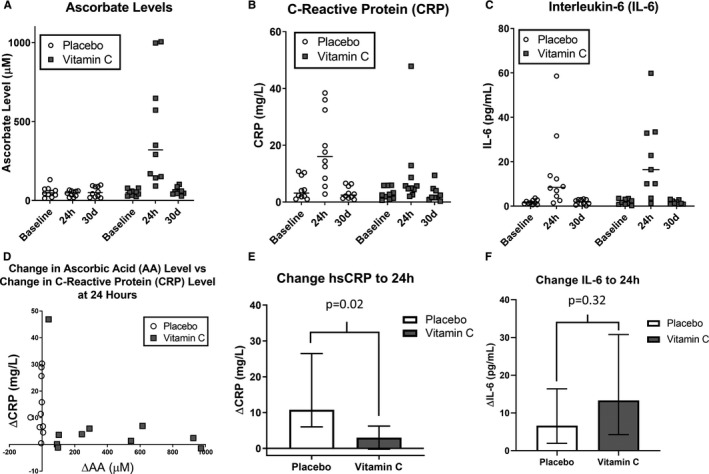
Background Catheter ablation is an effective treatment for atrial fibrillation (AF), but high levels of post-procedure inflammation predict adverse clinical events. Ascorbic acid (AA) has shown promise in reducing inflammation but is untested in this population. We sought to test the feasibility, safety, and preliminary effects on inflammatory biomarkers in the CITRIS-AF (Vitamin C Intravenous Treatment In the Setting of Atrial Fibrillation Ablation) pilot study. Methods and Results Patients scheduled to undergo AF ablation (N=20) were randomized 1:1 to double-blinded treatment with AA (200 mg/kg divided over 24 hours) or placebo. C-reactive protein and interleukin-6 levels were obtained before the first infusion and repeated at 24 hours and 30 days. Pain levels within 24 hours and early recurrence of AF within 90 days were recorded. Median and interquartile range were aged 63 (56-70) years, 13 (65%) men, and 18 (90%) white. Baseline data were similar between the 2 groups except ejection fraction. Baseline C-reactive protein levels were 2.56 (1.47-5.87) mg/L and similar between groups (P=0.48). Change in C-reactive protein from baseline to 24 hours was +10.79 (+6.56-23.19) mg/L in the placebo group and +3.01 (+0.40-5.43) mg/L in the AA group (P=0.02). Conversely, change in interleukin-6 was numerically higher in the AA group, though not statistically significant (P=0.32). One patient in each arm developed pericarditis; no adverse events related to the infusions were seen. There were no significant differences between aggregated post-procedure pain levels within 24 hours or early recurrence of AF (both P>0.05). Conclusions High-dose AA is safe and well tolerated at the time of AF ablation and may be associated with a blunted rise in C-reactive protein, although consistent findings were not seen in interleukin-6 levels. Further studies are needed to validate these findings and explore the potential benefit in improving clinically relevant outcomes. Clinical Trial Registration URL: http://www.clinicaltrials.gov. Unique identifier: NCT03148236.
Keywords: C‐reactive protein; ascorbic acid; atrial fibrillation; catheter ablation; inflammation.
Figures
References
-
- Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, Akar JG, Badhwar V, Brugada J, Camm J, Chen PS, Chen SA, Chung MK, Cosedis Nielsen J, Curtis AB, Davies DW, Day JD, D'Avila A, Natasja De Groot NMS, Di Biase L, Duytschaever M, Edgerton JR, Ellenbogen KA, Ellinor PT, Ernst S, Fenelon G, Gerstenfeld EP, Haines DE, Haissaguerre M, Helm RH, Hylek E, Jackman WM, Jalife J, Kalman JM, Kautzner J, Kottkamp H, Kuck KH, Kumagai K, Lee R, Lewalter T, Lindsay BD, MacLe L, Mansour M, Marchlinski FE, Michaud GF, Nakagawa H, Natale A, Nattel S, Okumura K, Packer D, Pokushalov E, Reynolds MR, Sanders P, Scanavacca M, Schilling R, Tondo C, Tsao HM, Verma A, Wilber DJ, Yamane T. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14:e275–e444. - PMC - PubMed
-
- Lim HS, Schultz C, Dang J, Alasady M, Lau DH, Brooks AG, Wong CX, Roberts‐Thomson KC, Young GD, Worthley MI, Sanders P, Willoughby SR. Time course of inflammation, myocardial injury, and prothrombotic response after radiofrequency catheter ablation for atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7:83–89. - PubMed
-
- Andrade JG, Khairy P, Verma A, Guerra PG, Dubuc M, Rivard L, Deyell MW, Mondesert B, Thibault B, Talajic M, Roy D, Macle L. Early recurrence of atrial tachyarrhythmias following radiofrequency catheter ablation of atrial fibrillation. Pacing Clin Electrophysiol. 2012;35:106–116. - PubMed
-
- Pignatelli P, Tanzilli G, Carnevale R, Di Santo S, Loffredo L, Celestini A, Proietti M, Tovaglia P, Mangieri E, Basili S, Violi F. Ascorbic acid infusion blunts CD40L upregulation in patients undergoing coronary stent. Cardiovasc Ther. 2011;29:385–394. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
