

Predicting Cardiovascular Outcomes by Baseline Lipoprotein(a) Concentrations: A Large Cohort and Long-Term Follow-up Study on Real-World Patients Receiving Percutaneous Coronary Intervention
- PMID: 32013705
- PMCID: PMC7033882
- DOI: 10.1161/JAHA.119.014581
Predicting Cardiovascular Outcomes by Baseline Lipoprotein(a) Concentrations: A Large Cohort and Long-Term Follow-up Study on Real-World Patients Receiving Percutaneous Coronary Intervention
Abstract
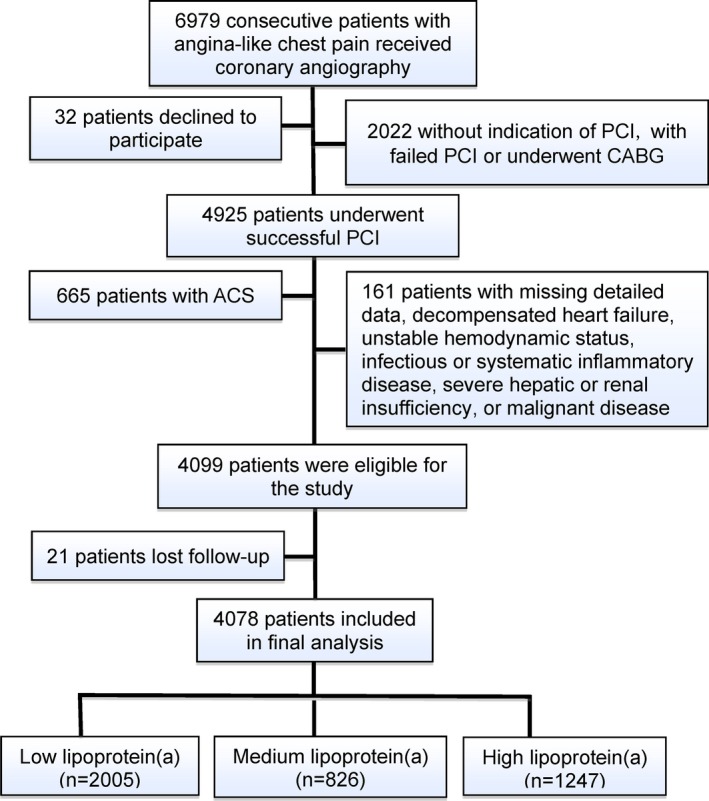
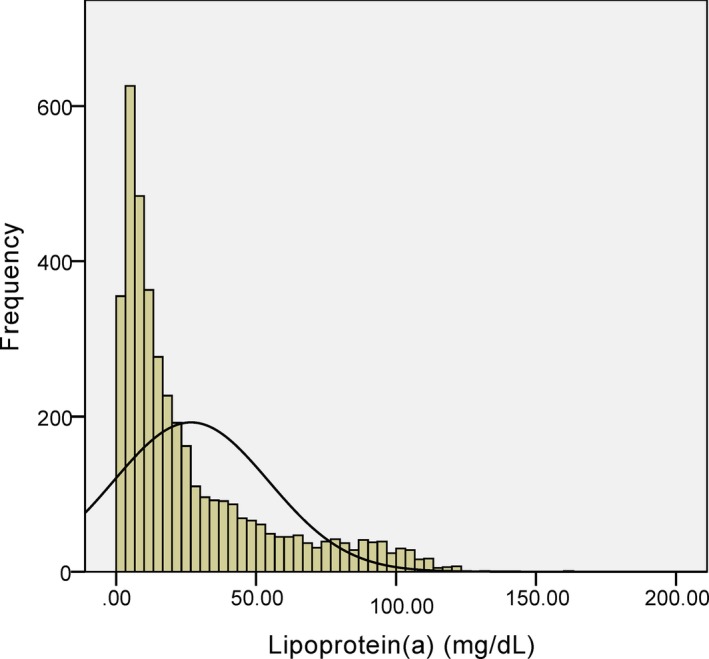
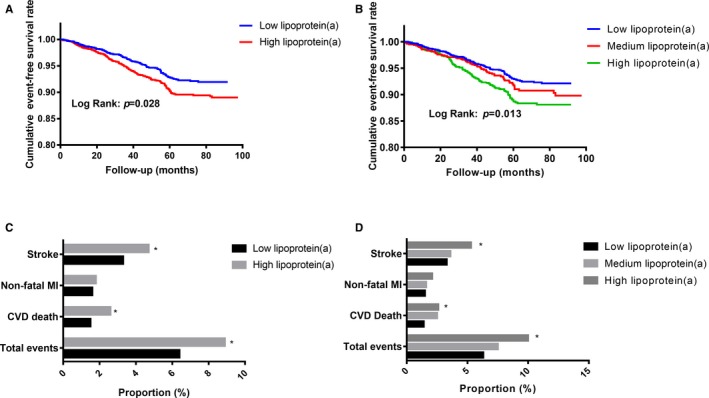
Background Although several studies have indicated that lipoprotein(a) is a useful prognostic predictor for patients following percutaneous coronary intervention (PCI), previous observations have somewhat been limited by either small sample size or short-term follow-up. Hence, this study aimed to evaluate the impact of lipoprotein(a) on long-term outcomes in a large cohort of stable coronary artery disease patients after PCI. Methods and Results In this multicenter and prospective study, we consecutively enrolled 4078 stable coronary artery disease patients undergoing PCI from March 2011 to March 2016. They were categorized according to both the median of lipoprotein(a) levels and lipoprotein(a) values of <15 (low), 15 to 30 (medium), and ≥30 mg/dL (high). All patients were followed up for occurrence of cardiovascular events, including cardiovascular death, nonfatal myocardial infarction, and stroke. During an average of 4.9 years of follow-up, 315 (7.7%) cardiovascular events occurred. The events group had significantly higher lipoprotein(a) levels than the nonevents group. Compared with the low lipoprotein(a) group, Kaplan-Meier analysis showed that the high lipoprotein(a) group had a significantly lower cumulative event-free survival rate, and multivariate Cox regression analysis further revealed that the high lipoprotein(a) group had significantly increased cardiovascular events risk. Moreover, adding continuous or categorical lipoprotein(a) to the Cox model led to a significant improvement in C-statistic, net reclassification, and integrated discrimination. Conclusions With a large sample size and long-term follow-up, our data confirmed that high lipoprotein(a) levels could be associated with a poor prognosis after PCI in stable coronary artery disease patients, suggesting that lipoprotein(a) measurements may be useful for patient risk stratification before selective PCI.
Keywords: cardiovascular events; coronary artery disease; lipoprotein(a); percutaneous coronary intervention.
Figures
References
-
- Garg S, Serruys PW. Coronary stents: current status. J Am Coll Cardiol. 2010;56(10 Suppl):S1–S42. - PubMed
-
- Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344:1383–1389. - PubMed
-
- Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, Joyal SV, Hill KA, Pfeffer MA, Skene AM; Pravastatin or Atorvastatin Evaluation and Infection Therapy‐Thrombolysis in Myocardial Infarction 22 Investigators. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1504. - PubMed
-
- Fearon WF, Nishi T, De Bruyne B, Boothroyd DB, Barbato E, Tonino P, Juni P, Pijls NHJ, Hlatky MA, Investigators FT. Clinical outcomes and cost‐effectiveness of fractional flow reserve‐guided percutaneous coronary intervention in patients with stable coronary artery disease: three‐year follow‐up of the FAME 2 trial (fractional flow reserve versus angiography for multivessel evaluation). Circulation. 2018;137:480–487. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
