

Consensus-Based Management Protocol (CREVICE Protocol) for the Treatment of Severe Traumatic Brain Injury Based on Imaging and Clinical Examination for Use When Intracranial Pressure Monitoring Is Not Employed
- PMID: 32013721
- PMCID: PMC7249475
- DOI: 10.1089/neu.2017.5599
Consensus-Based Management Protocol (CREVICE Protocol) for the Treatment of Severe Traumatic Brain Injury Based on Imaging and Clinical Examination for Use When Intracranial Pressure Monitoring Is Not Employed
Abstract
Globally, intracranial pressure (ICP) monitoring use in severe traumatic brain injury (sTBI) is inconsistent and susceptible to resource limitations and clinical philosophies. For situations without monitoring, there is no published comprehensive management algorithm specific to identifying and treating suspected intracranial hypertension (SICH) outside of the one ad hoc Imaging and Clinical Examination (ICE) protocol in the Benchmark Evidence from South American Trials: Treatment of Intracranial Pressure (BEST:TRIP) trial. As part of an ongoing National Institutes of Health (NIH)-supported project, a consensus conference involving 43 experienced Latin American Intensivists and Neurosurgeons who routinely care for sTBI patients without ICP monitoring, refined, revised, and augmented the original BEST:TRIP algorithm. Based on BEST:TRIP trial data and pre-meeting polling, 11 issues were targeted for development. We used Delphi-based methodology to codify individual statements and the final algorithm, using a group agreement threshold of 80%. The resulting CREVICE (Consensus REVised ICE) algorithm defines SICH and addresses both general management and specific treatment. SICH treatment modalities are organized into tiers to guide treatment escalation and tapering. Treatment schedules were developed to facilitate targeted management of disease severity. A decision-support model, based on the group's combined practices, is provided to guide this process. This algorithm provides the first comprehensive management algorithm for treating sTBI patients when ICP monitoring is not available. It is intended to provide a framework to guide clinical care and direct future research toward sTBI management. Because of the dearth of relevant literature, it is explicitly consensus based, and is provided solely as a resource (a "consensus-based curbside consult") to assist in treating sTBI in general intensive care units in resource-limited environments.
Keywords: ICP monitoring, intracranial hypertension; global health; neurocritical care; sTBI.
Conflict of interest statement
No competing financial interests exist.
Figures

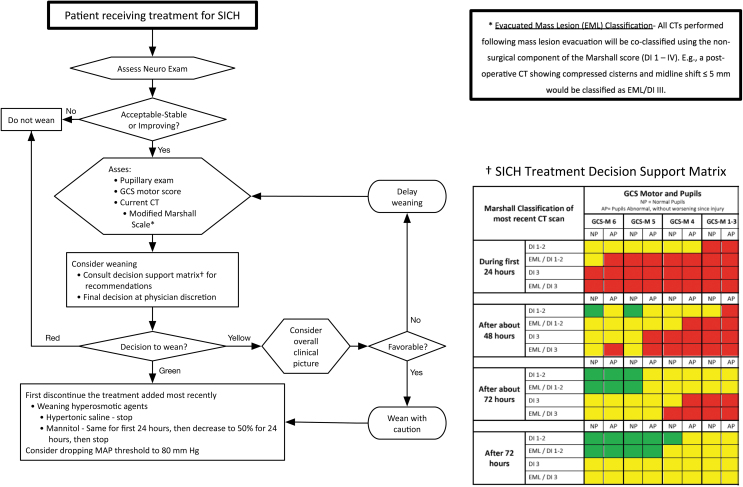
Green: it is recommended to begin to taper therapy.
Red: it is recommended not to taper therapy.
Yellow: this represents an intermediate status, wherein tapering therapy may be considered, but caution is recommended. The treating physician may choose to begin decreasing therapy, not to do so at that time, or to get more information to help in the decision. The decision to begin tapering treatment in patients in the “yellow” category should be accompanied by close observation as to the success of that decision.
References
-
- Aiolfi A., Khor D., Cho J., Benjamin E., Inaba K., and Demetriades D. (2018). Intracranial pressure monitoring in severe blunt head trauma: does the type of monitoring device matter? J. Neurosurg, 128, 828–833 - PubMed
-
- Hesdorffer D.C., and Ghajar J. (2007). Marked improvement in adherence to traumatic brain injury guidelines in United States trauma centers. J. Trauma 63, 841–848 - PubMed
-
- Myburgh J.A., Cooper D.J., Finfer S.R., Venkatesh B., Jones D., Higgins A., Bishop N., and Higlett T. (2008). Epidemiology and 12-month outcomes from traumatic brain injury in australia and new zealand. J. Trauma 64, 854–862 - PubMed
-
- Sahjpaul R., and Girotti M. (2000). Intracranial pressure monitoring in severe traumatic brain injury—results of a Canadian survey. Can. J. Neurol. Sci. 27, 143–147 - PubMed
-
- Stocchetti N., Penny K.I., Dearden M., Braakman R., Cohadon F., Iannotti F., Lapierre F., Karimi A., Maas A. Jr., Murray G.D., Ohman J., Persson L., Servadei F., Teasdale G.M., Trojanowski T., and Unterberg A. (2001). Intensive care management of head-injured patients in Europe: a survey from the European brain injury consortium. Intensive Care Med. 27, 400–406 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
