

The effect of vitamin D supplementation on hemoglobin concentration: a systematic review and meta-analysis
- PMID: 32013954
- PMCID: PMC6998164
- DOI: 10.1186/s12937-020-0526-3
The effect of vitamin D supplementation on hemoglobin concentration: a systematic review and meta-analysis
Erratum in
-
Correction to: The effect of vitamin D supplementation on hemoglobin concentration: a systematic review and meta-analysis.Nutr J. 2021 Mar 5;20(1):21. doi: 10.1186/s12937-021-00679-4. Nutr J. 2021. PMID: 33663525 Free PMC article. No abstract available.
Abstract
Aims: The purpose of this review was to investigate the effect of vitamin D supplements on hemoglobin concentration in subjects aged 17.5-68 years old; using randomized controlled trials (RCTs).
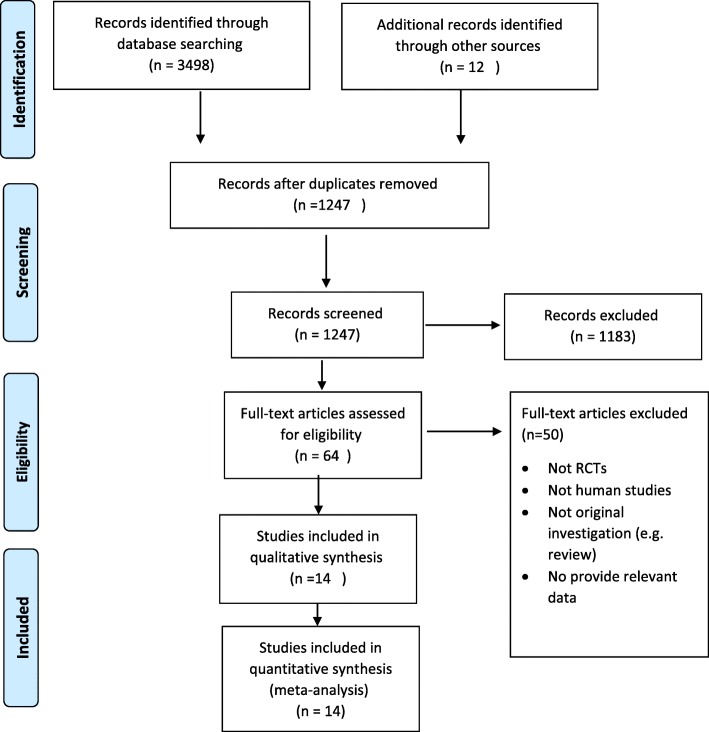
Methods: Relevant RCT studies were identified from January 2000 to January 2019 by using MeSH terms in PubMed, Embase, Cochrane Library, Clinical trials, Scopus databases and gray literature. The studies were reviewed systematically, and quality assessments were evaluated by the guidelines of the Cochrane risk of bias. The effect of vitamin D supplements (n = 14) on hemoglobin concentration was considered as primary outcome, while its effects on the levels of ferritin, transferrin saturation and iron status were derived as secondary outcomes. In total, 1385 subjects with age range of 17.5 to 68 years old were examined for 3 h to 6 months; Mean (standard deviation) or median interquartile changes in the hemoglobin concentration in each treatment group was recorded for meta-analysis.
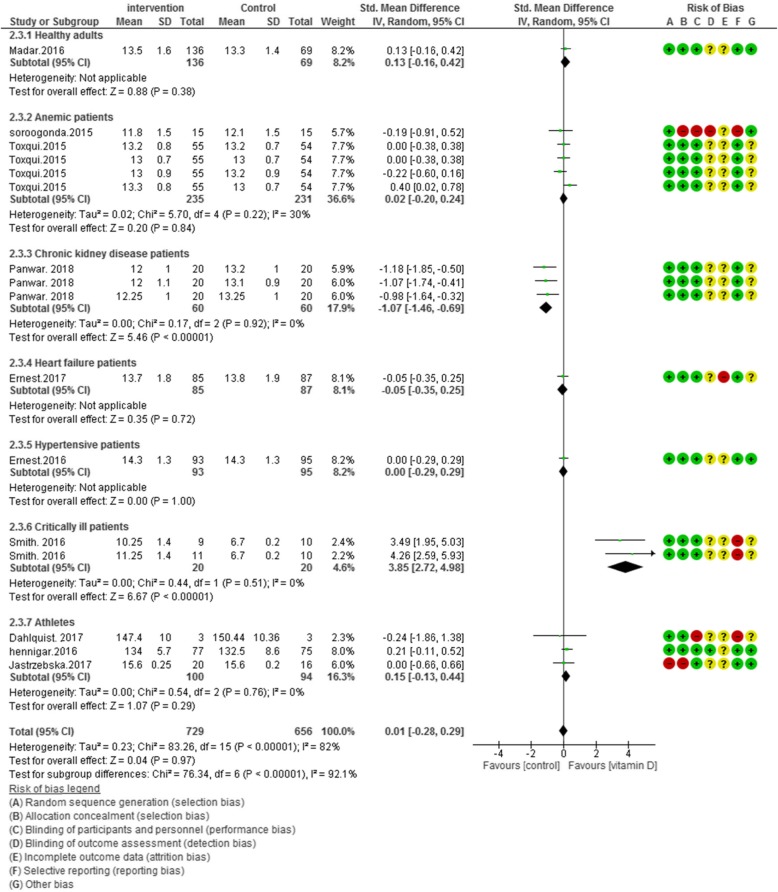
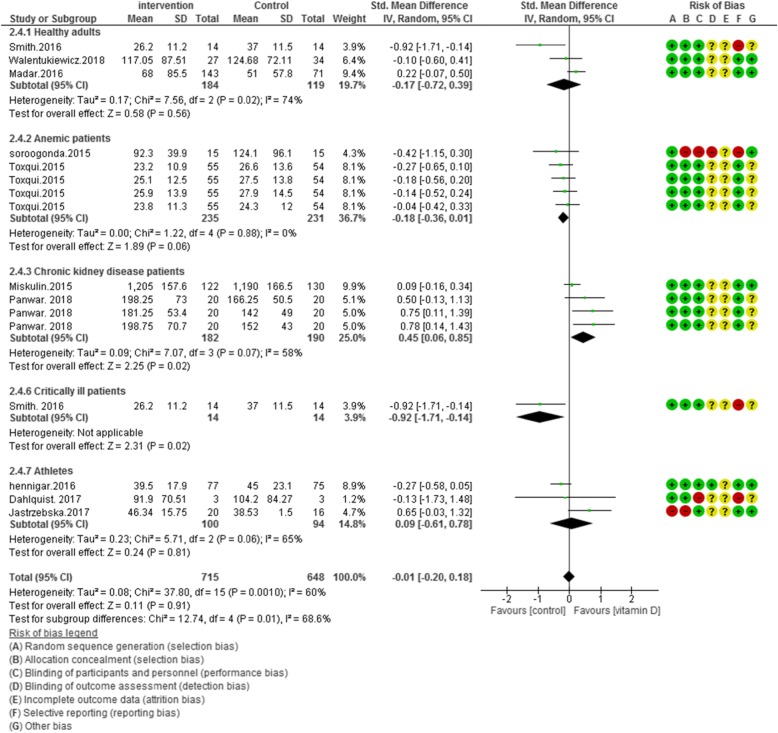
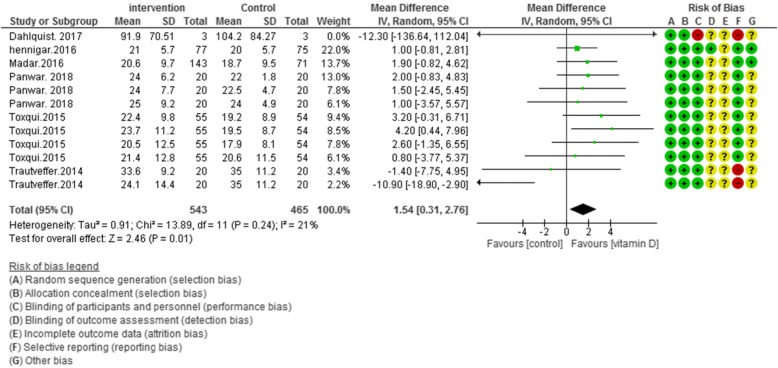
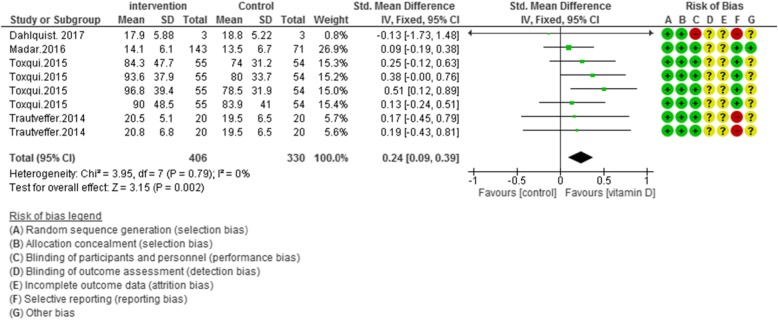
Results: Fourteen RCTs met the inclusion criteria. Current study findings propose that vitamin D supplementation leads to a non-significant reduction in hemoglobin levels in subjects (17.5-68 years old) [std. mean difference (SMD): 0.01; 95% CI: - 0.28, 0.29; P = 0.95], also it has no significant effect on ferritin concentrations [std. mean difference (SMD): -0.01; 95% CI: [- 0.20, 0.18; P = 0.91]. However, vitamin D supplementation demonstrated positive effects on transferrin saturation [mean difference (MD): 1.54; 95% CI: 0.31, 2.76; P = 0.01] and iron status [std. mean difference (SMD): 0.24; 95% CI: - 0.09, 0.39; P = 0.002].
Conclusion: Current review concluded that supplementation with vitamin D had no significant effect on hemoglobin and ferritin levels while positive effects on transferrin saturation and iron status were observed. Further clinical studies are required to determine the actual effect of this intervention on hemoglobin levels.
Keywords: Anemia; Hemoglobin; Iron status; RCT; Vitamin D.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Meta-analysis of vitamin D supplementation and hemoglobin concentration: methodological faults obscure the interpretation of the data.Nutr J. 2021 Mar 19;20(1):22. doi: 10.1186/s12937-021-00681-w. Nutr J. 2021. PMID: 33740966 Free PMC article.
-
Vitamin D supplementation and hemoglobin: dosing matters in prevention/treatment of anemia.Nutr J. 2021 Mar 19;20(1):23. doi: 10.1186/s12937-021-00680-x. Nutr J. 2021. PMID: 33740996 Free PMC article. No abstract available.
-
Reply to: vitamin D supplementation and hemoglobin: dosing matters in prevention/treatment of anemia.Nutr J. 2021 Apr 8;20(1):33. doi: 10.1186/s12937-021-00683-8. Nutr J. 2021. PMID: 33832484 Free PMC article. No abstract available.
-
Reply to: Meta-analysis of vitamin D supplementation and hemoglobin concentration: methodological faults obscure the interpretation of the data.Nutr J. 2021 Apr 8;20(1):34. doi: 10.1186/s12937-021-00682-9. Nutr J. 2021. PMID: 33832491 Free PMC article. No abstract available.
References
-
- Hershko C, Hoffbrand AV, Keret D, Souroujon M, Maschler I, Monselise Y, et al. Role of autoimmune gastritis, Helicobacter pylori and celiac disease in refractory or unexplained iron deficiency anemia. Haematologica. 2005;90(5):585–595. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
