

Effectiveness of a new sensorized videolaryngoscope for retraining on neonatal intubation in simulation environment
- PMID: 32014009
- PMCID: PMC6998091
- DOI: 10.1186/s13052-020-0774-z
Effectiveness of a new sensorized videolaryngoscope for retraining on neonatal intubation in simulation environment
Abstract
Background: In recent years, medical training has significantly increased the use of simulation for teaching and evaluation. The retraining of medical personnel in Italy is entrusted to the program of Continuous Education in Medicine, mainly based on theoretical training. The aim of this study is to assess whether the use of a new sensorized platform for the execution of the neonatal intubation procedure in simulation environment can complement theoretical retraining of experienced health professionals.
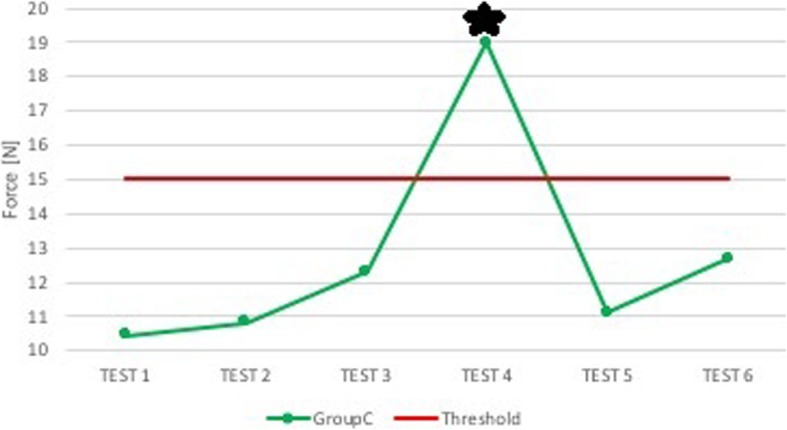
Methods: Neonatal intubation tests were performed using a commercial manikin and a modified video-laryngoscope by the addition of force and position sensors, which provide the user with feedback when the threshold is exceeded. Two categories carried out the simulation tests: anesthesiologists and pediatricians. The categories were divided into three groups each, and various configurations were tested: the first group of both specialists carried out the tests without feedback (i.e. control groups, gr. A and A1), the second groups received sound and visual feedback from the instrument (gr. B and B1) and the third ones had also the support of a physician expert in the use of the instrument (gr. C and C1). The instrumentation used by pediatricians was provided in a playful form, including a game with increasing difficulty levels.
Results: Both in the case with feedback only and in the case with humans support, anesthesiologists did not show a specific trend of improvement. Pediatricians, in comparison with anesthesiologists, showed a positive reaction to both the presence of feedback and that of experienced personnel. Comparing the performance of the two control groups, the two categories of experienced doctors perform similar forces. Pediatricians enjoyed the "Level Game", through which they were able to test and confront themselves, trying to improve their own performance.
Conclusions: Our instrument is more effective when is playful and competitive, introducing something more than just a sound feedback, and allowing training by increasing levels. It is more effective if the users can adapt their own technique to the instrument by themselves, without any external help.
Keywords: Neonatal intubation; Retraining; Sensorized; Simulation; Skill trainer.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures












References
-
- Santalucia P, Ingrassia PL, Zaninelli A, Ragazzoni L, Ganau A, Gensini GF. La simulazione in medicina. J Ital Med Educ. 2016;70:3166–3169.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
