

Kaposiform hemangioendothelioma: current knowledge and future perspectives
- PMID: 32014025
- PMCID: PMC6998257
- DOI: 10.1186/s13023-020-1320-1
Kaposiform hemangioendothelioma: current knowledge and future perspectives
Abstract
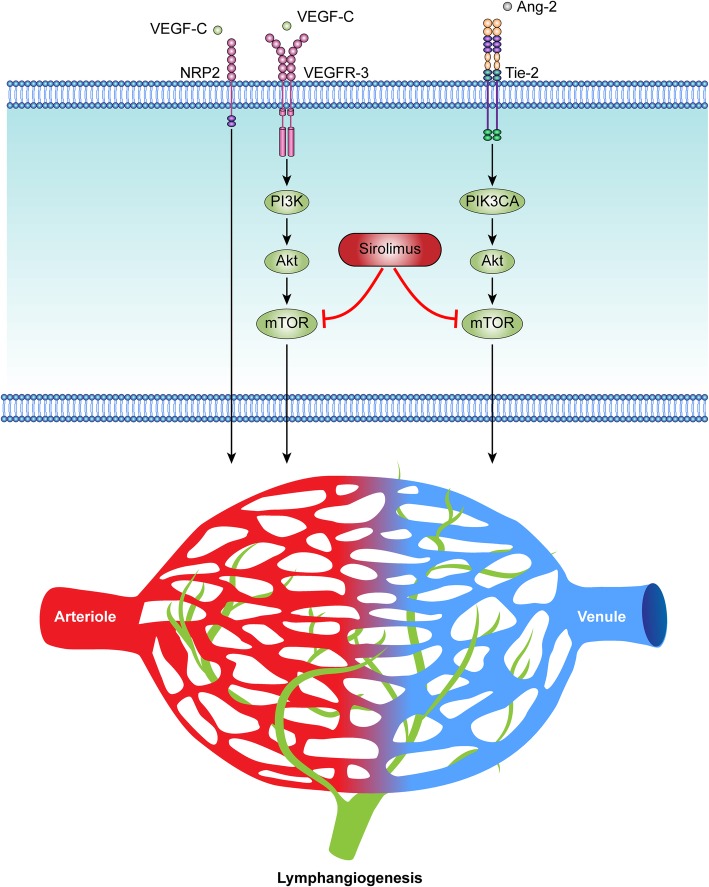
Kaposiform hemangioendothelioma (KHE) is a rare vascular neoplasm with high morbidity and mortality. The initiating mechanism during the pathogenesis of KHE has yet to be discovered. The main pathological features of KHE are abnormal angiogenesis and lymphangiogenesis. KHEs are clinically heterogeneous and may develop into a life-threatening thrombocytopenia and consumptive coagulopathy, known as the Kasabach-Merritt phenomenon (KMP). The heterogeneity and the highly frequent occurrence of disease-related comorbidities make the management of KHE challenging. Currently, there are no medications approved by the FDA for the treatment of KHE. Multiple treatment regimens have been used with varying success, and new clinical trials are in progress. In severe patients, multiple agents with variable adjuvant therapies are given in sequence or in combination. Recent studies have demonstrated a satisfactory efficacy of sirolimus, an inhibitor of mammalian target of rapamycin, in the treatment of KHE. Novel targeted treatments based on a better understanding of the pathogenesis of KHE are needed to maximize patient outcomes and quality of life. This review summarizes the epidemiology, etiology, pathophysiology, clinical features, diagnosis and treatments of KHE. Recent new concepts and future perspectives for KHE will also be discussed.
Keywords: Angiogenesis; Kaposiform hemangioendothelioma; Kasabach-Merritt phenomenon; Lymphangiogenesis; Treatment.
Conflict of interest statement
The authors declare that they have no competing interests, either financial or non-financial, that could be perceived as prejudicing the impartiality of the research reported.
Figures







References
-
- Lyons LL, North PE, Mac-Moune LF, Stoler MH, Folpe AL, Weiss SW. Kaposiform hemangioendothelioma: a study of 33 cases emphasizing its pathologic, immunophenotypic, and biologic uniqueness from juvenile hemangioma. Am J Surg Pathol. 2004;28(5):559–568. doi: 10.1097/00000478-200405000-00001. - DOI - PubMed
-
- Fernandez-Pineda I, Lopez-Gutierrez JC, Chocarro G, Bernabeu-Wittel J, Ramirez-Villar GL. Long-term outcome of vincristine-aspirin-ticlopidine (VAT) therapy for vascular tumors associated with kasabach-Merritt phenomenon. Pediatr Blood Cancer. 2013;60(9):1478–1481. doi: 10.1002/pbc.24543. - DOI - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
