

Fecal microbiota transplantation to maintain remission in Crohn's disease: a pilot randomized controlled study
- PMID: 32014035
- PMCID: PMC6998149
- DOI: 10.1186/s40168-020-0792-5
Fecal microbiota transplantation to maintain remission in Crohn's disease: a pilot randomized controlled study
Abstract
Background: The role of the gut microbiota in Crohn's disease (CD) is established and fecal microbiota transplantation (FMT) is an attractive therapeutic strategy. No randomized controlled clinical trial results are available. We performed a randomized, single-blind, sham-controlled pilot trial of FMT in adults with colonic or ileo-colonic CD.
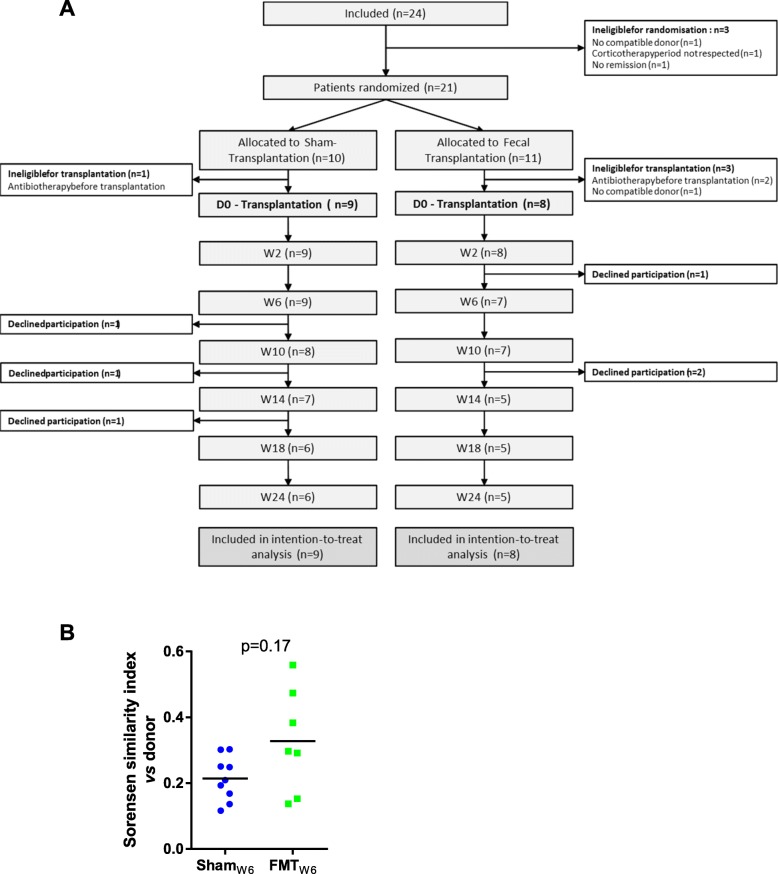
Method: Patients enrolled while in flare received oral corticosteroid. Once in clinical remission, patients were randomized to receive either FMT or sham transplantation during a colonoscopy. Corticosteroids were tapered and a second colonoscopy was performed at week 6. The primary endpoint was the implantation of the donor microbiota at week 6 (Sorensen index > 0.6).
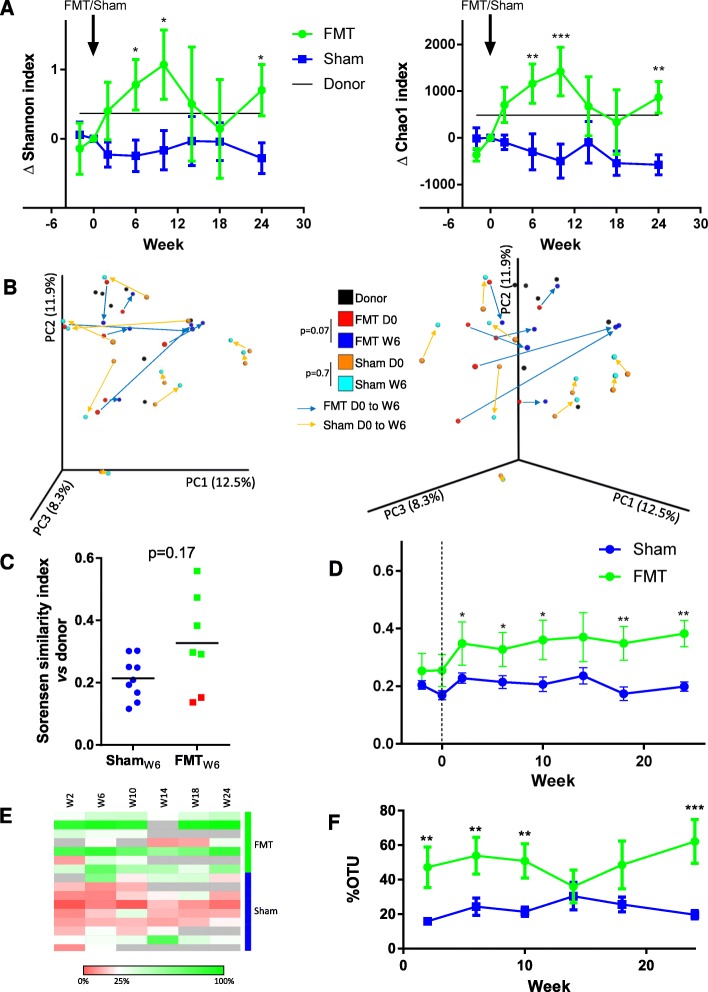
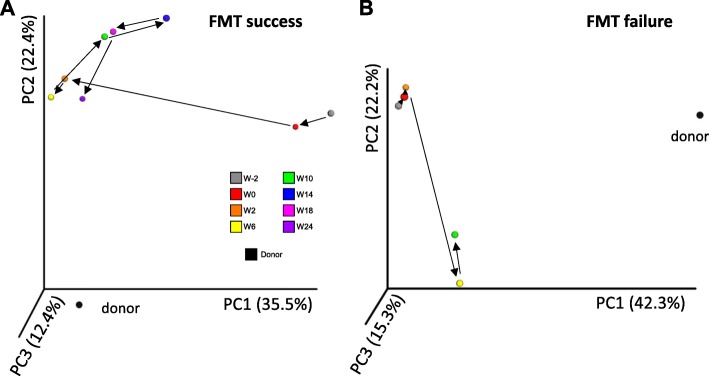
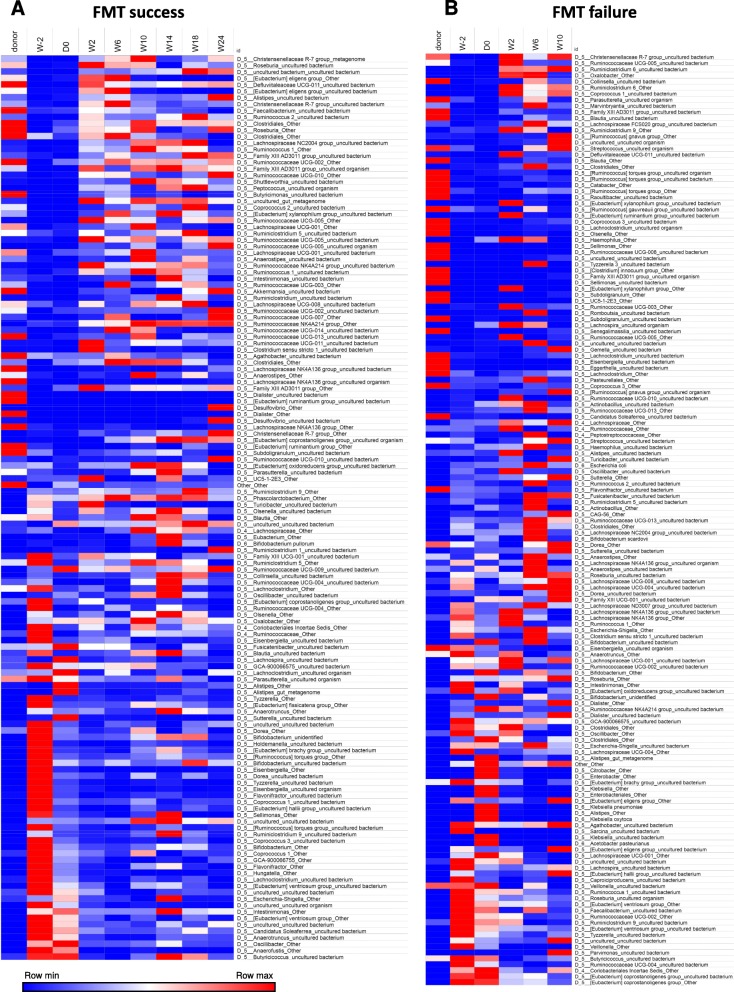
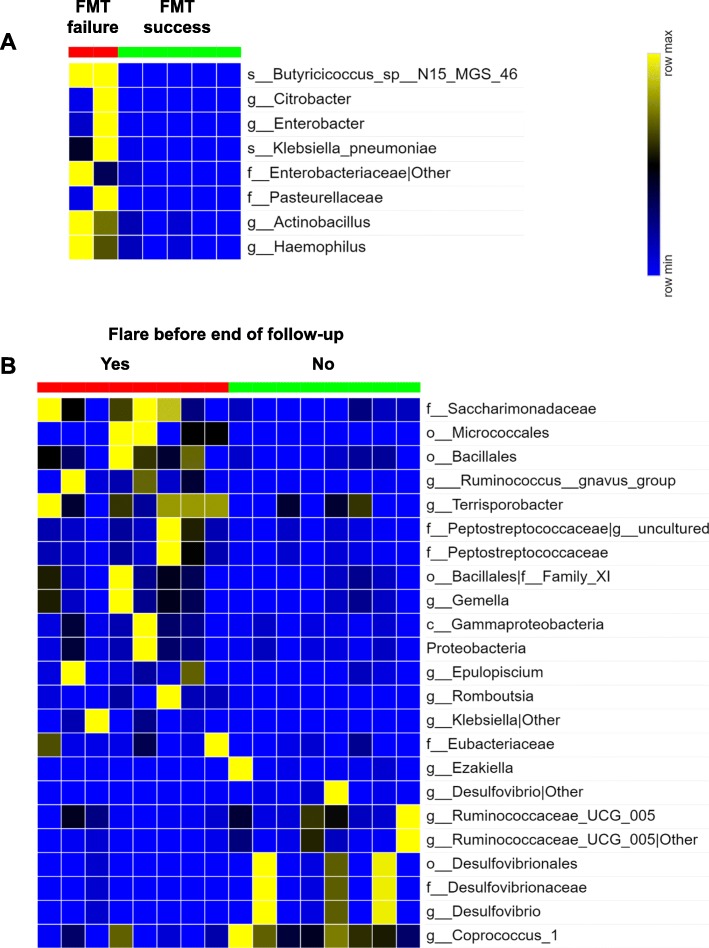
Results: Eight patients received FMT and nine sham transplantation. None of the patients reached the primary endpoint. The steroid-free clinical remission rate at 10 and 24 weeks was 44.4% (4/9) and 33.3% (3/9) in the sham transplantation group and 87.5% (7/8) and 50.0% (4/8; one patient loss of follow-up while in remission at week 12 and considered in flare at week 24) in the FMT group. Crohn's Disease Endoscopic Index of Severity decreased 6 weeks after FMT (p = 0.03) but not after sham transplantation (p = 0.8). Conversely, the CRP level increased 6 weeks after sham transplantation (p = 0.008) but not after FMT (p = 0.5). Absence of donor microbiota engraftment was associated with flare. No safety signal was identified.
Conclusion: The primary endpoint was not reached for any patient. In this pilot study, higher colonization by donor microbiota was associated with maintenance of remission. These results must be confirmed in larger studies (NCT02097797). Video abstract.
Keywords: Crohn’s disease; Fecal microbiota transplantation; Randomized controlled trial.
Conflict of interest statement
HS received unrestricted study grants from Danone, Biocodex, and Enterome; board membership, consultancy, or lecture fees from Carenity, Abbvie, Astellas, Danone, Ferring, Mayoly Spindler, MSD, Novartis, Roche, Tillots, Enterome, Maat, BiomX, Biose, Novartis, and Takeda; and a co-funder of Exeliom bioscience. TS received unrestricted study grants from Amgen, AstraZeneca, Bayer, BMS, Boehringer-Ingelheim, Daiichi-Sankyo, Eli-Lilly, MSD, Pfizer, and Sanofi; and board membership, consultancy, or lecture fees from AstraZeneca, Astellas, BMS, MSD, Novartis, Sanofi, and Pfizer. The other authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
