

Impact of a posttraumatic cerebral infarction on outcome in patients with TBI: the Italian multicenter cohort INCEPT study
- PMID: 32014041
- PMCID: PMC6998281
- DOI: 10.1186/s13054-020-2746-5
Impact of a posttraumatic cerebral infarction on outcome in patients with TBI: the Italian multicenter cohort INCEPT study
Abstract
Background: Post-traumatic cerebral infarction (PTCI) is common after traumatic brain injury (TBI). It is unclear what the occurrence of a PTCI is, how it impacts the long-term outcome, and whether it adds incremental prognostic value to established outcome predictors.
Methods: This was a prospective multicenter cohort study of moderate and severe TBI patients. The primary objective was to evaluate if PTCI was an independent risk factor for the 6-month outcome assessed with the Glasgow Outcome Scale (GOS). We also assessed the PTCI occurrence and if it adds incremental value to the International Mission for Prognosis and Clinical Trial design in TBI (IMPACT) core and extended models.
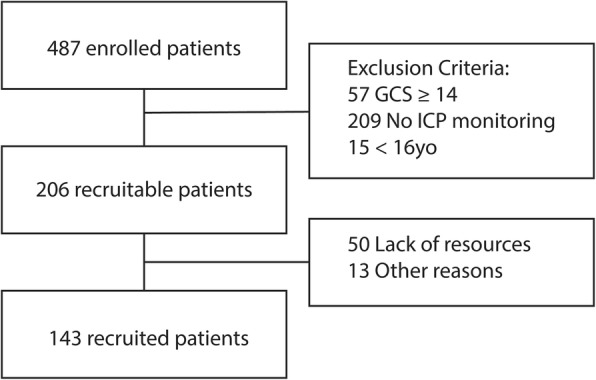
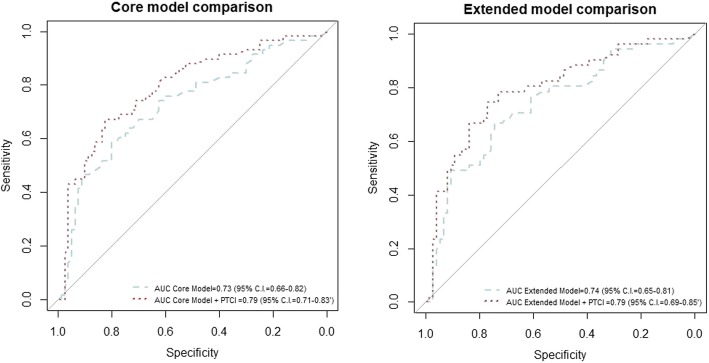
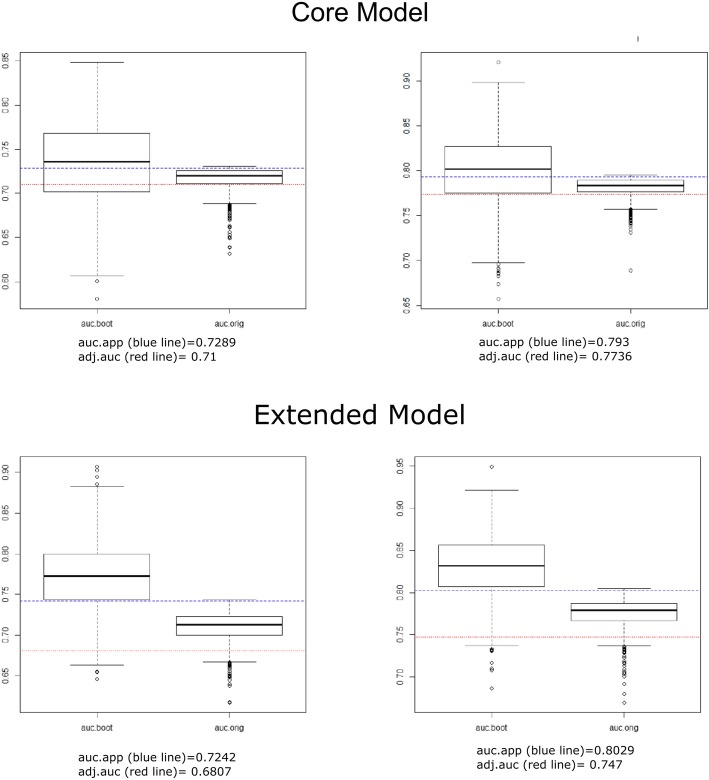
Results: We enrolled 143 patients, of whom 47 (32.9%) developed a PTCI. In the multiple ordered logistic regression, PTCI was retained in both the core and extended IMPACT models as an independent predictor of the GOS. The predictive performances increased significantly when PTCI was added to the IMPACT core model (AUC = 0.73, 95% C.I. 0.66-0.82; increased to AUC = 0.79, 95% CI 0.71-0.83, p = 0.0007) and extended model (AUC = 0.74, 95% C.I. 0.65-0.81 increased to AUC = 0.80, 95% C.I. 0.69-0.85; p = 0.00008). Patients with PTCI showed higher ICU mortality and 6-month mortality, whereas hospital mortality did not differ between the two groups.
Conclusions: PTCI is a common complication in patients suffering from a moderate or severe TBI and is an independent risk factor for long-term disability. The addition of PTCI to the IMPACT core and extended predictive models significantly increased their performance in predicting the GOS.
Trial registration: The present study was registered in ClinicalTrial.gov with the ID number NCT02430324.
Keywords: Disability; Long term outcome; Posttraumatic cerebral infarction; Traumatic brain injury.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
