

ESR1 mutations are frequent in newly diagnosed metastatic and loco-regional recurrence of endocrine-treated breast cancer and carry worse prognosis
- PMID: 32014063
- PMCID: PMC6998824
- DOI: 10.1186/s13058-020-1246-5
ESR1 mutations are frequent in newly diagnosed metastatic and loco-regional recurrence of endocrine-treated breast cancer and carry worse prognosis
Erratum in
-
Correction to: ESR1 mutations are frequent in newly diagnosed metastatic and loco-regional recurrence of endocrine-treated breast cancer and carry worse prognosis.Breast Cancer Res. 2020 Mar 12;22(1):28. doi: 10.1186/s13058-020-01265-y. Breast Cancer Res. 2020. PMID: 32164744 Free PMC article.
Abstract
Background: Emerging mutations in the ESR1 gene that encodes for the estrogen receptor (ER) are associated with resistance to endocrine therapy. ESR1 mutations rarely exist in primary tumors (~ 1%) but are relatively common (10-50%) in metastatic, endocrine therapy-resistant cancers and are associated with a shorter progression-free survival. Little is known about the incidence and clinical implication of these mutations in early recurrence events, such as local recurrences or newly diagnosed metastatic disease.
Methods: We collected 130 archival tumor samples from 103 breast cancer patients treated with endocrine therapy prior to their local/metastatic recurrence. The cohort consisted of 41 patients having at least 1 sample from local/loco-regional recurrence and 62 patients with metastatic disease (of whom 41 newly diagnosed and 28 with advanced disease). The 5 most common ESR1 hotspot mutations (D538G, L536R, Y537S/N/C) were analyzed either by targeted sequencing or by droplet digital PCR. Progression-free survival (PFS), disease-free survival (DFS), and distant recurrence-free survival (DRFS) were statistically tested by Kaplan-Meier analysis.
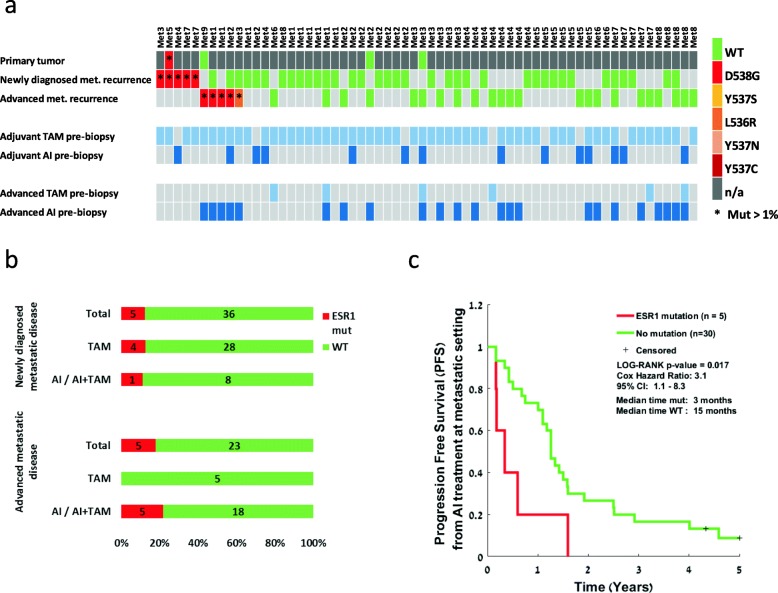
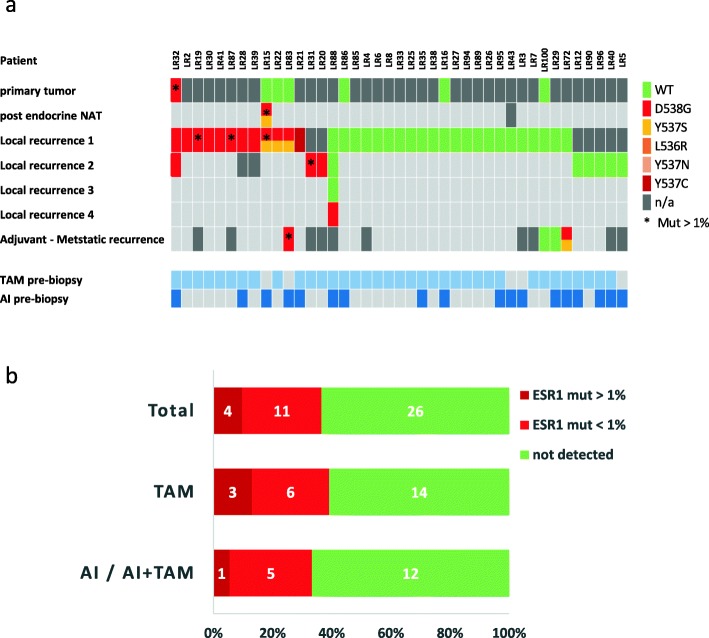
Results: The prevalence of ESR1 mutations was 5/41 (12%) in newly diagnosed metastatic patients and 5/28 (18%) for advanced metastases, detected at allele frequency > 1%. All mutations in advanced metastases were detected in patients previously treated with both tamoxifen (TAM) and aromatase inhibitors (AI). However, in newly diagnosed metastatic patients, 4/5 mutations occurred in patients treated with TAM alone. PFS on AI treatment in metastatic patients was significantly shorter for ESR1 mutation carriers (p = 0.017). In the local recurrence cohort, ESR1 mutations were identified in 15/41 (36%) patients but only 4/41 (10%) were detected at allele frequency > 1%. Again, most mutations (3/4) were detected under TAM monotherapy. Notably, 1 patient developed ESR1 mutation while on neoadjuvant endocrine therapy. DFS and DRFS were significantly shorter (p = 0.04 and p = 0.017, respectively) in patients that had ESR1 mutations (> 1%) in their loco-regional recurrence tumor.
Conclusions: Clinically relevant ESR1 mutations are prevalent in newly diagnosed metastatic and local recurrence of endocrine-treated breast cancer. Since local recurrences are amenable to curative therapy, these mutations may inform the selection of subsequent endocrine therapies.
Keywords: Breast cancer; ESR1 mutation; Endocrine treatment; Loco-regional/local recurrence; Metastasis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Richman J, Dowsett M. Beyond 5 years: enduring risk of recurrence in oestrogen receptor-positive breast cancer. Nat Rev Clin Oncol. 2019;16(5):296-311. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
