

Immunotherapy of Pediatric Solid Tumors: Treatments at a Crossroads, with an Emphasis on Antibodies
- PMID: 32015013
- PMCID: PMC7058412
- DOI: 10.1158/2326-6066.CIR-19-0692
Immunotherapy of Pediatric Solid Tumors: Treatments at a Crossroads, with an Emphasis on Antibodies
Abstract
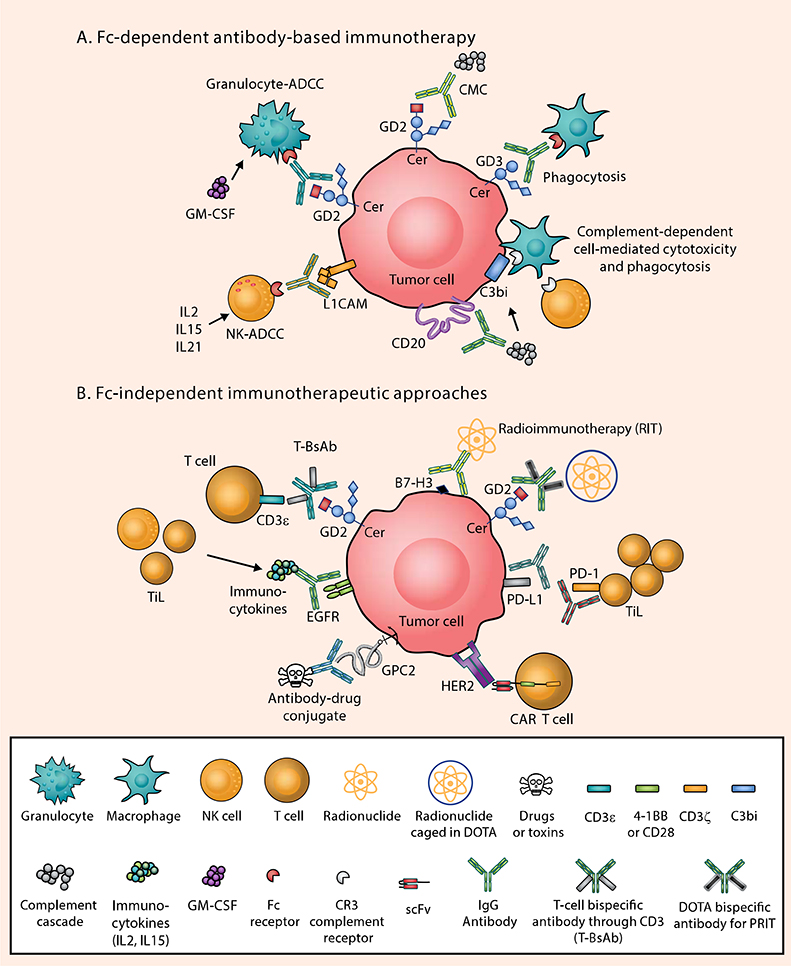
Over the last decade, immunotherapy has rapidly changed the therapeutic landscape and prognosis for many hematologic malignancies and adult solid tumors. Despite this success, immunotherapy for pediatric solid tumors remains in the early stages of development, and significant clinical benefit has yet to be realized, with anti-GD2 for neuroblastoma being the exception. The limited neoepitope expression and paucity of T-cell infiltration into the immunosuppressive tumor microenvironment have hampered current established immunotherapies. Emerging approaches to recruit T cells, to convert phenotypically "cold" into "inflamed" tumors, and to vastly improve therapeutic indices hold exceptional promise. Here, we review these approaches, highlighting the role of the tumor microenvironment and novel antibody platforms to maximize the full clinical potential of immunotherapy in pediatric oncology.
©2020 American Association for Cancer Research.
Figures
References
-
- Cheung NK, Cheung IY, Kushner BH, Ostrovnaya I, Chamberlain E, Kramer K, et al. Murine Anti-GD2 Monoclonal Antibody 3F8 Combined With Granulocyte-Macrophage Colony-Stimulating Factor and 13-Cis-Retinoic Acid in High-Risk Patients With Stage 4 Neuroblastoma in First Remission. J Clin Oncol 2012;30(26):3264–70 doi 10.1200/JCO.2011.41.3807. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
