

Changes in inflammatory and vasoactive mediator profiles during valvular surgery with or without infective endocarditis: A case control pilot study
- PMID: 32015566
- PMCID: PMC6996967
- DOI: 10.1371/journal.pone.0228286
Changes in inflammatory and vasoactive mediator profiles during valvular surgery with or without infective endocarditis: A case control pilot study
Abstract
Background: More than 50% of patients with infective endocarditis (IE) develop an indication for surgery. Despite its benefit, surgery is associated with a high incidence of multiple organ dysfunction syndrome (MODS) and mortality, which may be linked to increased release of inflammatory mediators during cardiopulmonary bypass (CPB). We therefore assessed plasma cytokine profiles in patients undergoing valve surgery with or without IE.
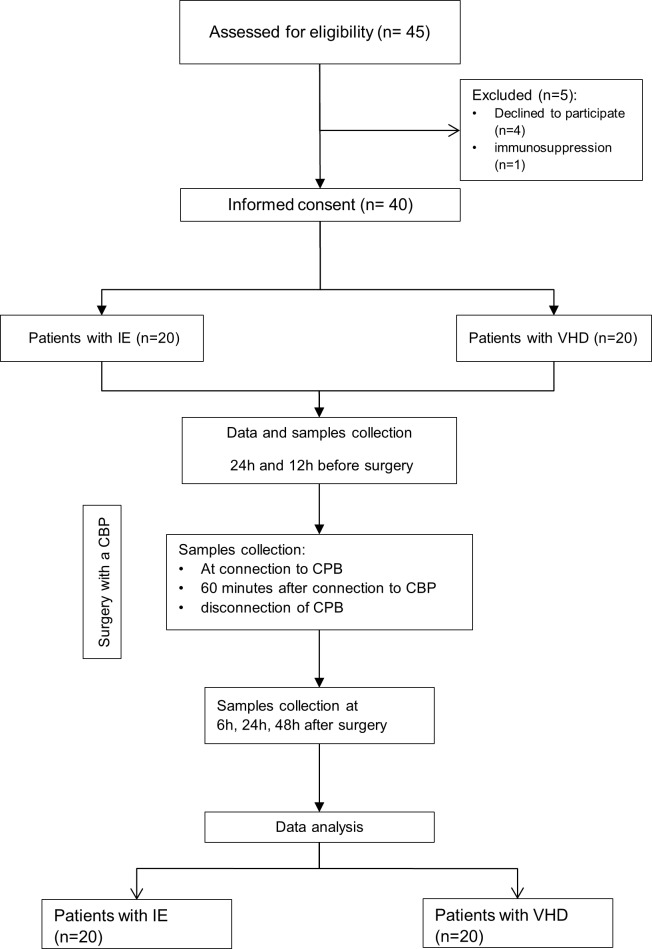
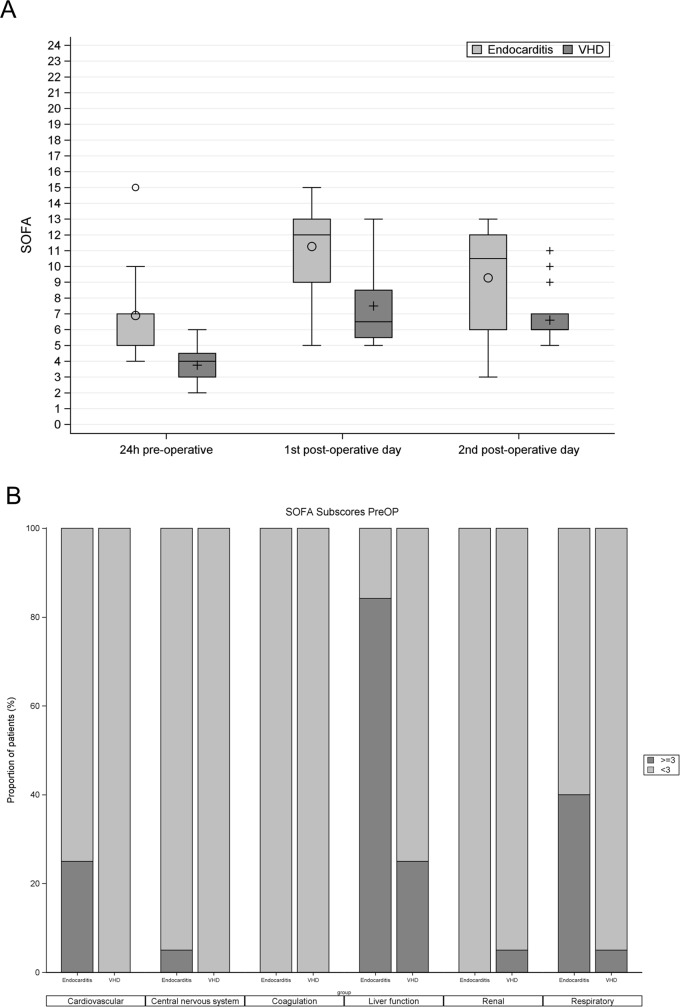
Methods: We performed a prospective case-control pilot study comparing patients undergoing cardiac valve surgery with or without IE. Plasma profiles of inflammatory mediators were measured at 7 defined time points and reported as median (interquartile). The degree of MODS was measured using sequential organ failure assessment (SOFA) score.
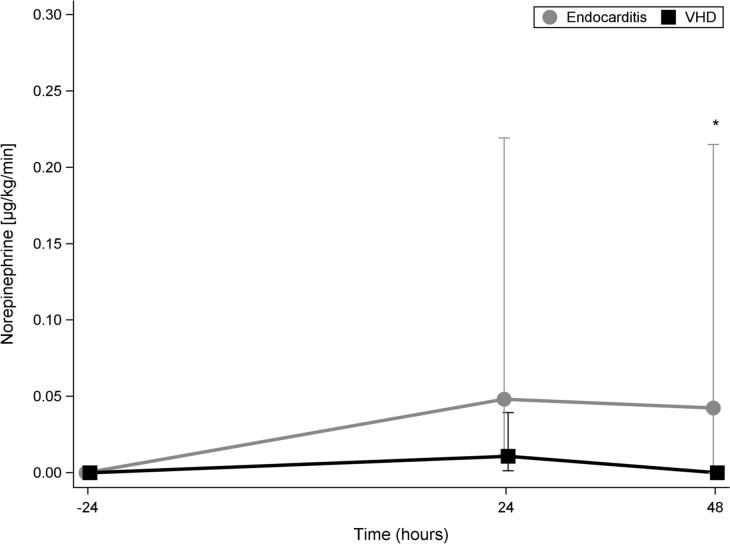
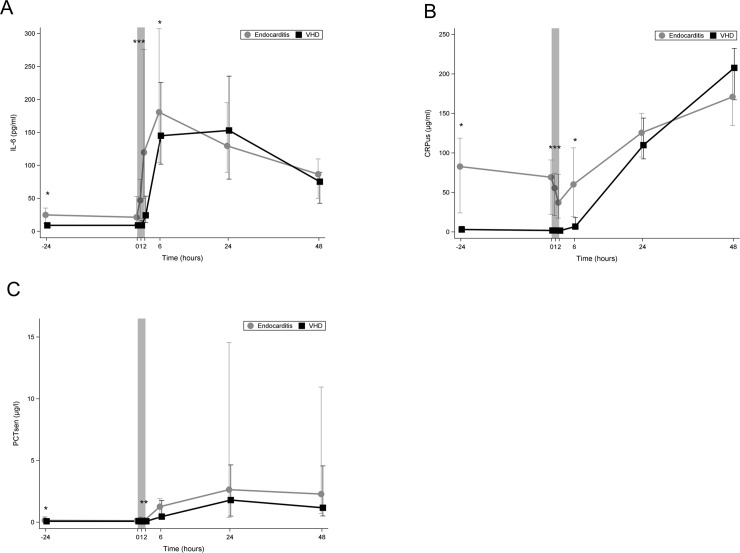
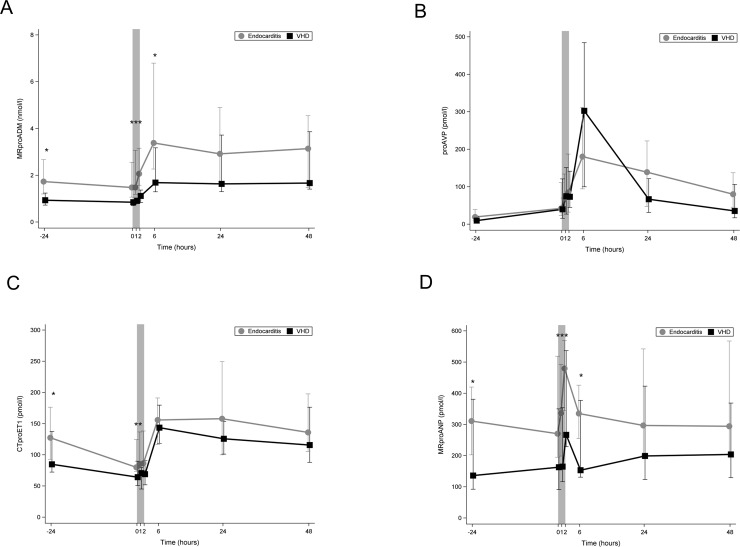
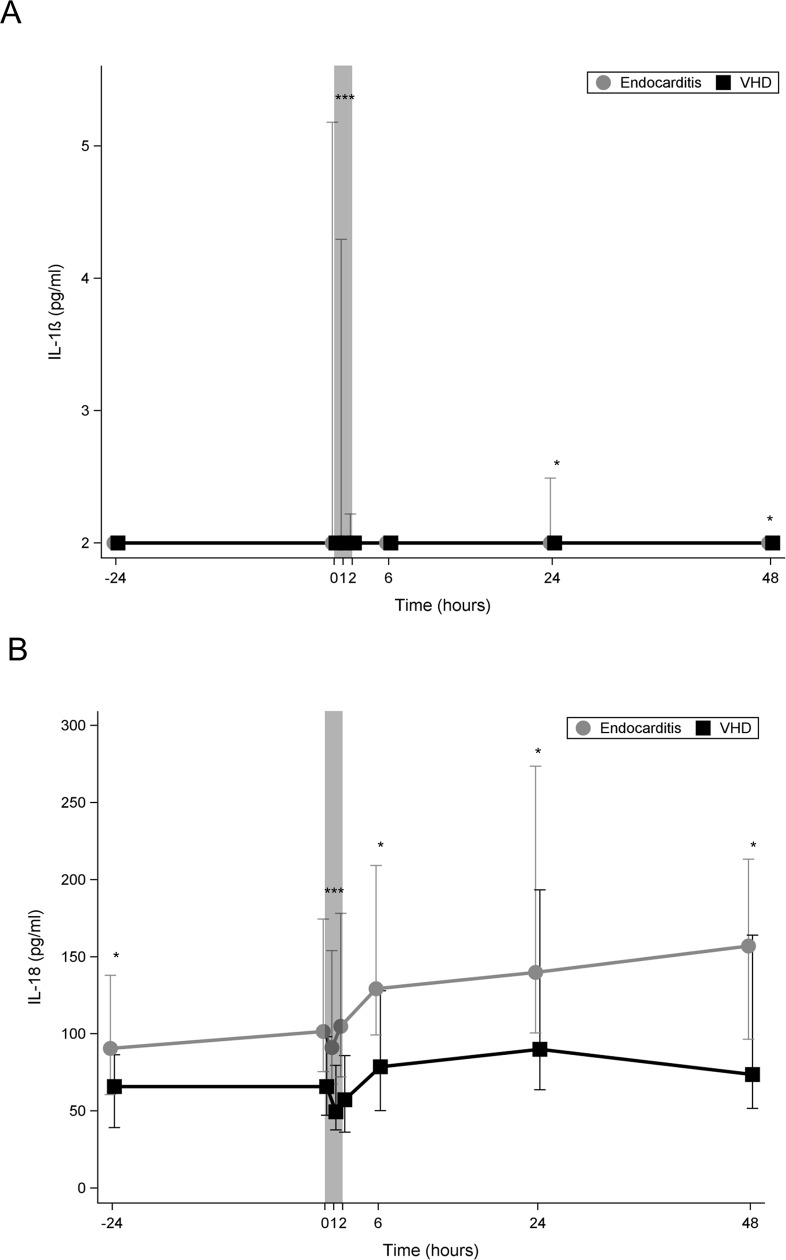
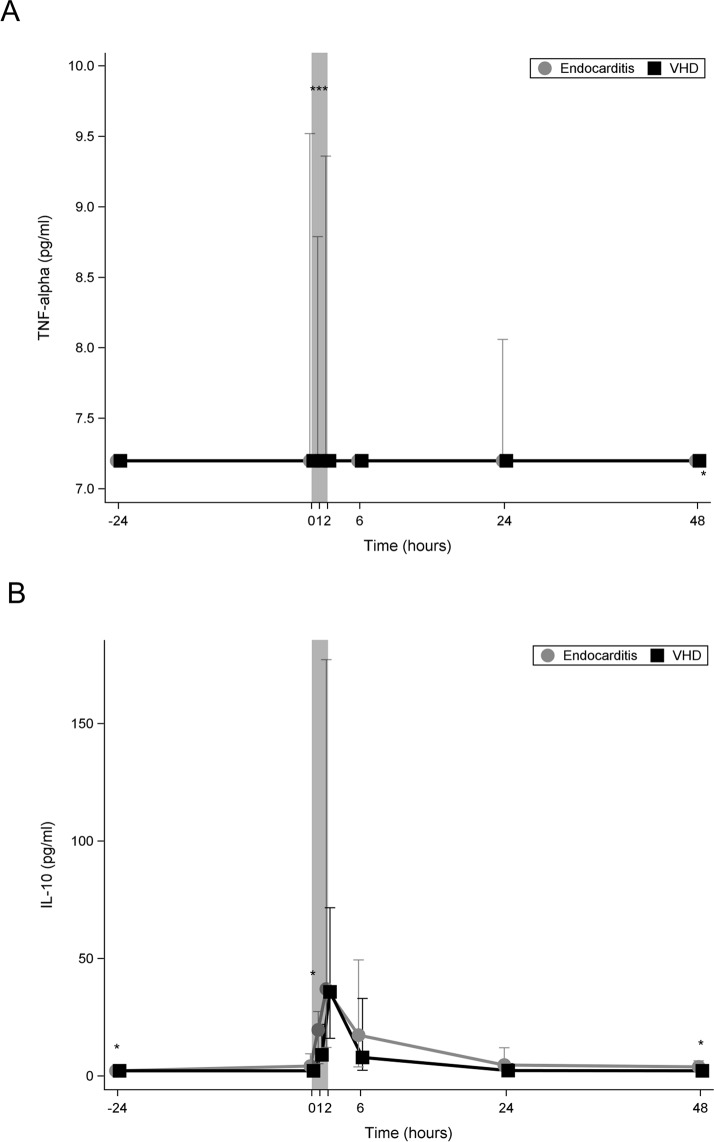
Results: Between May and December 2016 we included 40 patients (20 in each group). Both groups showed similar distribution of age and gender. Patients with IE had higher preoperative SOFA (6.9± 2.6 vs 3.8 ± 1.1, p<0.001) and operative risk scores (EuroSCORE II 18.6±17.4 vs. 1.8±1.3, p<0.001). In-hospital mortality was higher in IE patients (35% vs. 5%; p<0.001). Multiple organ failure was the cause of death in all non-survivors. At the end of CPB, median levels of following inflammatory mediators were higher in IE compared to control group: IL-6 (119.73 (226.49) vs. 24.48 (40.09) pg/ml, p = 0.001); IL-18 (104.82 (105.99) vs. 57.30 (49.53) pg/ml, p<0.001); Mid-regional pro-adrenomedullin (MR-proADM) (2.06 (1.58) vs. 1.11 (0.53) nmol/L, p = 0.003); MR- pro-atrial natriuretic peptide (MR-proANP) (479.49 (224.74) vs. 266.55 (308.26) pmol/l, p = 0.028). IL-1β and TNF- α were only detectable in IE patients and first after starting CPB. Plasma levels of IL-6, IL-18, MRproADM, and MRproANP during CPB were significantly lower in survivors than in those who died.
Conclusion: The presence of infective endocarditis during cardiac valve surgery is associated with increased inflammatory response as evident by higher plasma cytokine levels and other inflammatory mediators. Actively reducing inflammatory response appears to be a plausible therapeutic concept.
Trial registration: ClinicalTrials.gov, ID: NCT02727413.
Conflict of interest statement
All other authors declare no competing interests
Figures
References
-
- Murdoch DR, Corey GR, Hoen B, Miro JM, Fowler VG Jr., Bayer AS, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Archives of internal medicine. 2009;169(5):463–73. 10.1001/archinternmed.2008.603 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
