

Editorial
doi: 10.21037/atm.2019.09.100.
More than just a screen to liberate from mechanical ventilation: treat to keep extubated?
Affiliations
- PMID: 32016056
- PMCID: PMC6976406
- DOI: 10.21037/atm.2019.09.100
Item in Clipboard
Editorial
More than just a screen to liberate from mechanical ventilation: treat to keep extubated?
Ann Transl Med.
2019 Dec.
No abstract available
Conflict of interest statement
Conflicts of Interest: Dr. Fink is Chief Science Officer for Aerogen Pharma Corp and discloses relationships with Dance Biopharm. Mr. Scott discloses relationship with Ventec Life Systems. The other authors have no conflicts of interest to declare.
Figures
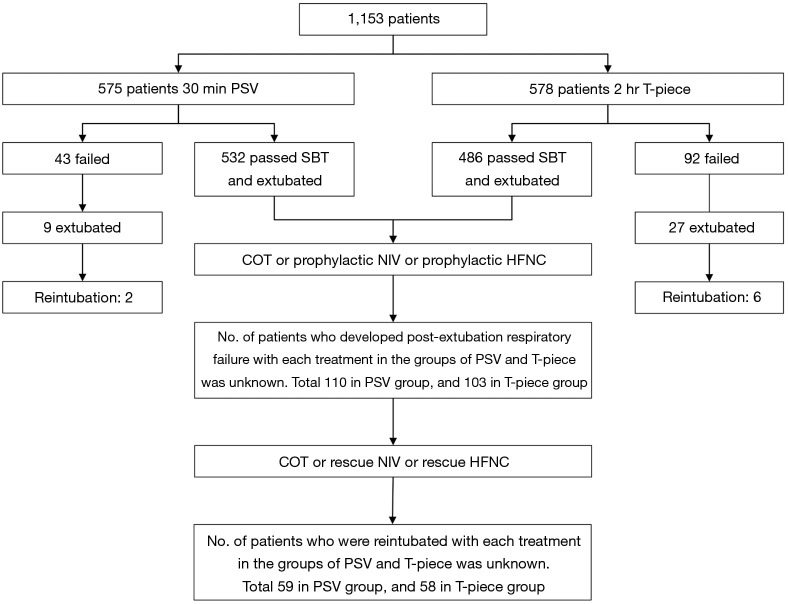
In the Subirà et al.’s study, among the 575 patients who were assigned to receive 30 min PSV SBT, 532 patients passed SBT and were extubated. The remaining 43 patients failed SBT, however 9 were still extubated. In those 541 extubated patients, 51 of them received prophylactic NIV and 91 received prophylactic HFNC. The exact number of patients who received prophylactic NIV and HFNC were unknown in the 532 patients who passed the SBT and were extubated. One hundred and ten in 532 patients developed post-extubation respiratory failure, but the number of patients in the groups of COT, prophylactic NIV and HFNC were unreported. For those 110 patients, some might have changed respiratory support devices, such as from COT to HFNC or NIV, or from HFNC to NIV, as a “rescue therapy”, 59 patients ended with reintubation. The number of patients in those rescue treatment groups were unknown. Similar situation also exists in the group of 2-hour T-piece SBT. NIV, noninvasive ventilation; HFNC, high-flow nasal cannula; COT, conventional oxygen therapy.
Comment on
-
Effect of Pressure Support vs T-Piece Ventilation Strategies During Spontaneous Breathing Trials on Successful Extubation Among Patients Receiving Mechanical Ventilation: A Randomized Clinical Trial.JAMA. 2019 Jun 11;321(22):2175-2182. doi: 10.1001/jama.2019.7234. JAMA. 2019. PMID: 31184740 Free PMC article. Clinical Trial.
References
Publication types
LinkOut - more resources
Full Text Sources