

Association Between Neurological Disorders and Death by Suicide in Denmark
- PMID: 32016308
- PMCID: PMC7042859
- DOI: 10.1001/jama.2019.21834
Association Between Neurological Disorders and Death by Suicide in Denmark
Abstract
Importance: Neurological disorders have been linked to suicide, but the risk across a broad spectrum of neurological disorders remains to be assessed.
Objectives: To examine whether people with neurological disorders die by suicide more often than other people and to assess for temporal associations.
Design, setting, and participants: Nationwide, retrospective cohort study on all persons 15 years or older living in Denmark, from 1980 through 2016 (N = 7 300 395).
Exposures: Medical contact for head injury, stroke, epilepsy, polyneuropathy, diseases of myoneural junction, Parkinson disease, multiple sclerosis, central nervous system infections, meningitis, encephalitis, amyotrophic lateral sclerosis, Huntington disease, dementia, intellectual disability, and other brain diseases from 1977 through 2016 (n = 1 248 252).
Main outcomes and measures: Death by suicide during 1980-2016. Adjusted incidence rate ratio (IRRs) were estimated using Poisson regressions, adjusted for sociodemographics, comorbidity, psychiatric diagnoses, and self-harm.
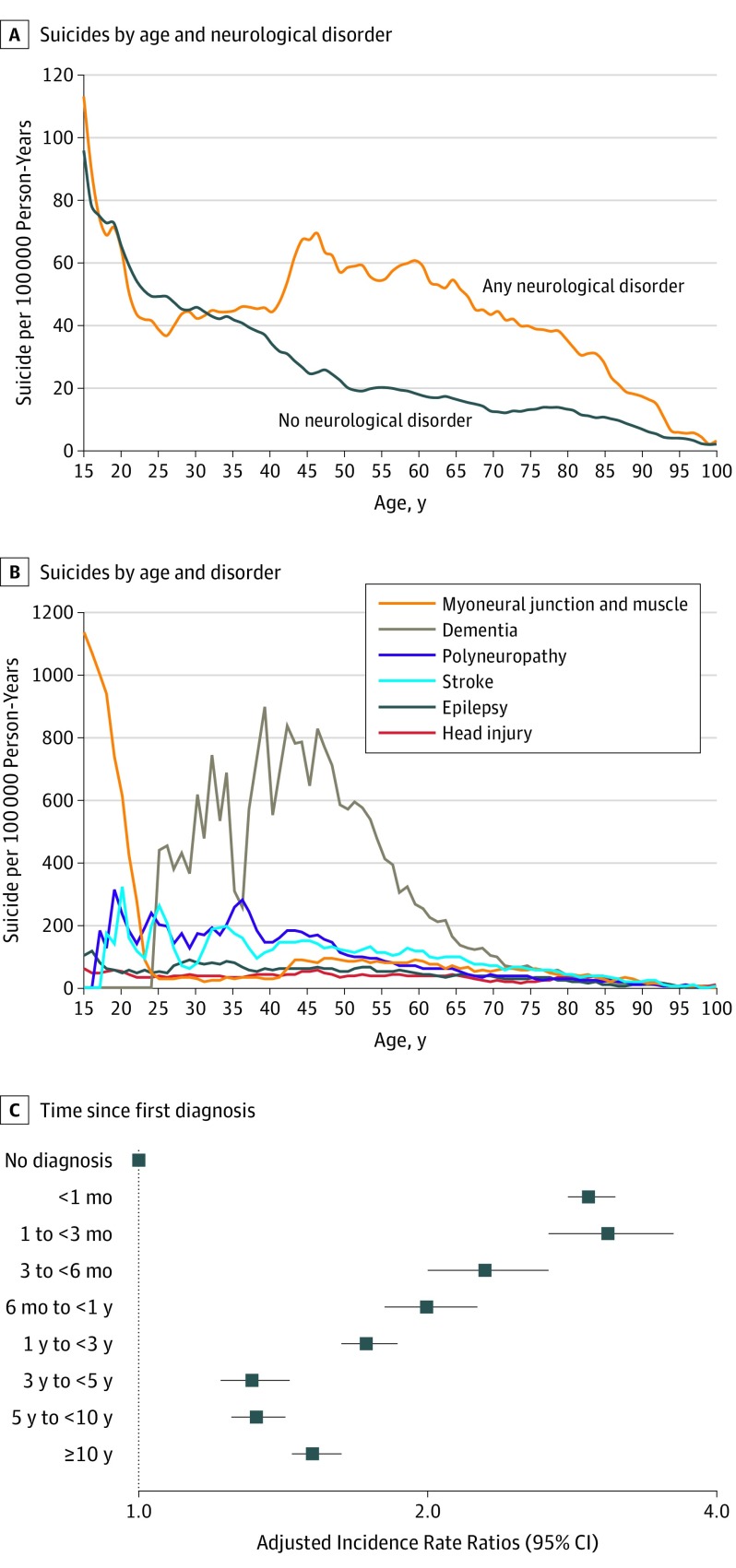
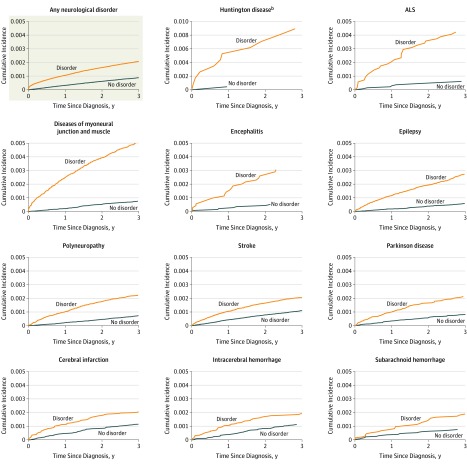
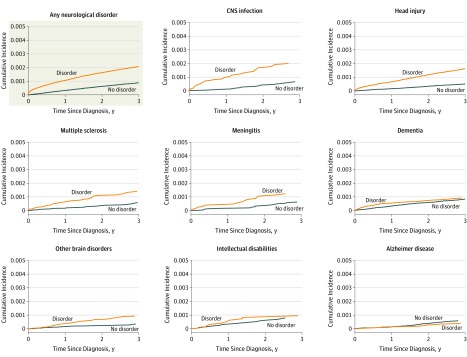
Results: Of the more than 7.3 million individuals observed over 161 935 233 person-years (49.1% males), 35 483 died by suicide (median duration of follow-up, 23.6 years; interquartile range, 10.0-37.0 years; mean age, 51.9 years; SD, 17.9 years). Of those, 77.4% were males, and 14.7% (n = 5141) were diagnosed with a neurological disorder, equivalent to a suicide rate of 44.0 per 100 000 person-years compared with 20.1 per 100 000 person-years among individuals not diagnosed with a neurological disorder. People diagnosed with a neurological disorder had an adjusted IRR of 1.8 (95% CI, 1.7-1.8) compared with those not diagnosed. The excess adjusted IRRs were 4.9 (95% CI, 3.5-6.9) for amyotrophic lateral sclerosis, 4.9 (95% CI, 3.1-7.7) for Huntington disease, 2.2 (95% CI, 1.9-2.6) for multiple sclerosis, 1.7 (95% CI, 1.6-1.7) for head injury, 1.3 (95% CI, 1.2-1.3) for stroke, and 1.7 (95% CI, 1.6-1.8) for epilepsy. The association varied according to time since diagnosis with an adjusted IRR for 1 to 3 months of 3.1 (95% CI, 2.7-3.6) and for 10 or more years, 1.5 (95% CI, 1.4 to 1.6, P < .001). Compared with those who were not diagnosed with a neurological disorder, those with dementia had a lower overall adjusted IRR of 0.8 (95% CI, 0.7-0.9), which was elevated during the first month after diagnosis to 3.0 (95% CI, 1.9-4.6; P < .001). The absolute risk of suicide for people with Huntington disease was 1.6% (95% CI, 1.0%-2.5%).
Conclusions and relevance: In Denmark from 1980 through 2016, there was a significantly higher rate of suicide among those with a diagnosed neurological disorder than persons not diagnosed with a neurological disorder. However, the absolute risk difference was small.
Conflict of interest statement
Figures
References
-
- Stenager EN, Stenager E. Disease, Pain and Suicidal Behavior. New York, NY: Haworth Medical Press; 1997.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
