

Resection of the gastric submucosal tumor (G-SMT) originating from the muscularis propria layer: comparison of efficacy, patients' tolerability, and clinical outcomes between endoscopic full-thickness resection and surgical resection
- PMID: 32016516
- PMCID: PMC7394934
- DOI: 10.1007/s00464-019-07311-x
Resection of the gastric submucosal tumor (G-SMT) originating from the muscularis propria layer: comparison of efficacy, patients' tolerability, and clinical outcomes between endoscopic full-thickness resection and surgical resection
Abstract
Background and aims: Endoscopic full-thickness resection (EFTR) has been increasingly applied in the treatment of gastric submucosal tumors (G-SMTs) with explorative intention. This study aimed to compare the efficacy, tolerability, and clinical outcomes of EFTR and surgical intervention for the management of muscularis propria (MP)-derived G-SMTs.
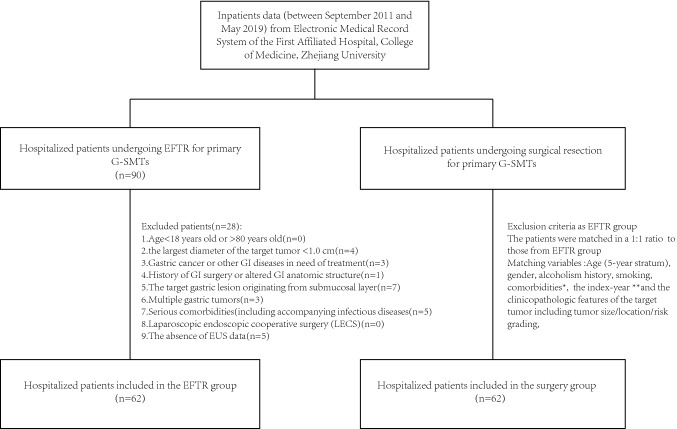
Methods: Between September 2011 and May 2019, the clinical records of patients with MP-derived G-SMTs undergoing EFTR at our endoscopic unit were collected. A cohort of people with primary MP-derived G-SMTs treated by surgery was matched in a 1:1 ratio to EFTR group with regard to patients' baseline characteristics, clinicopathologic features of the tumor and the procedure date. The perioperative outcomes and follow-up data were analyzed.
Results: In total, 62 and 62 patients were enrolled into the surgery and EFTR group, respectively, with median follow-up of 786 days. The size of G-SMTs (with ulceration) ranged from 10 to 90 mm. For patients with tumor smaller than 30 mm, surgery and EFTR group presented comparable procedural success rate (both were 100%), en bloc resection rate (100% vs. 94.7%), tumor capsule rupture rate (0% vs. 5.3%), and pathological R0 resection rate (both were 100%). EFTR had a statistically significant advantage over surgery for estimated blood loss (3.12 ± 5.20 vs. 46.97 ± 60.73 ml, p ≤ 0.001), discrepancy between the pre- and postprocedural hemoglobin level (5.18 ± 5.43 vs. 9.84 ± 8.25 g/L, p = 0.005), bowel function restoration [1 (0-5) vs. 3 (1-5) days, p ≤ 0.001], and hospital cost (28,617.09 ± 6720.78 vs. 33,963.10 ± 13,454.52 Yuan, p = 0.033). The patients with tumor larger than 30 mm showed roughly the same outcomes after comparison analysis of the two groups. However, the clinical data revealed lower en bloc resection rate (75.0% vs. 100%, p = 0.022) and higher tumor capsule rupture rate (25.0% vs. 0%, p = 0.022) for EFTR when compared to surgery. The procedure time, duration of postprocedural fasting and antibiotics usage, and hospital stay of the two groups were equivalent. The occurrence rate of adverse events within postoperative day 7 were 74.2% and 72.6% after EFTR and surgery, respectively (p = 1.000). No complications occurred during the follow-up.
Conclusion: For treatment of MP-derived G-SMTs (with or without ulceration), our study showed the feasibility and safety of EFTR, which also provided better results in terms of procedural blood loss, the postoperative bowel function restoration and cost-effectiveness when compared to surgery, whereas the surgery was superior in en bloc resection rate for G-SMTs larger than 30 mm. The postprocedural clinical outcomes seemed to be equivalent in these two resection methods.
Keywords: Endoscopic full-thickness resection (EFTR); Gastrointestinal stromal tumors (GIST); General surgery; Lamina propria; Laparoscopy; Postoperative complications.
Conflict of interest statement
Dr. Liu Sha, Dr. Zhou Xinxin, Dr. Yao Yongxing, Dr. Shi Keda, Dr. Yu Mosang, and Dr. Ji Feng have no conflicts of interest or financial ties to disclose.
Figures

References
-
- Zhou PH, Yao LQ, Qin XY, Cai MY, Xu MD, Zhong YS, Chen WF, Zhang YQ, Qin WZ, Hu JW, Liu JZ. Endoscopic full-thickness resection without laparoscopic assistance for gastric submucosal tumors originated from the muscularis propria. Surg Endosc. 2011;25(9):2926–2931. - PubMed
-
- Cai MY, Martin Carreras-Presas F, Zhou PH. Endoscopic full-thickness resection for gastrointestinal submucosal tumors. Dig Endosc. 2018;30(Suppl 1):17–24. - PubMed
-
- Fritscher-Ravens A, Cuming T, Jacobsen B, Seehusen F, Ghanbari A, Kahle E, von Herbay A, Koehler P, Milla P. Feasibility and safety of endoscopic full-thickness esophageal wall resection and defect closure: a prospective long-term survival animal study. Gastrointest Endosc. 2009;69(7):1314–1320. - PubMed
-
- Dray X, Giday SA, Buscaglia JM, Gabrielson KL, Kantsevoy SV, Magno P, Assumpcao L, Shin EJ, Reddings SK, Woods KE, Marohn MR, Kalloo AN. Omentoplasty for gastrotomy closure after natural orifice transluminal endoscopic surgery procedures (with video) Gastrointest Endosc. 2009;70(1):131–140. - PubMed
-
- Suzuki H, Ikeda K. Endoscopic mucosal resection and full thickness resection with complete defect closure for early gastrointestinal malignancies. Endoscopy. 2001;33(5):437–439. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
