

Implementation of cisternostomy as adjuvant to decompressive craniectomy for the management of severe brain trauma
- PMID: 32016585
- PMCID: PMC7046565
- DOI: 10.1007/s00701-020-04222-y
Implementation of cisternostomy as adjuvant to decompressive craniectomy for the management of severe brain trauma
Abstract
Objective: To evaluate the value of an adjuvant cisternostomy (AC) to decompressive craniectomy (DC) for the management of patients with severe traumatic brain injury (sTBI).
Methods: A single-center retrospective quality control analysis of a consecutive series of sTBI patients surgically treated with AC or DC alone between 2013 and 2018. A subgroup analysis, "primary procedure" and "secondary procedure", was also performed. We examined the impact of AC vs. DC on clinical outcome, including long-term (6 months) extended Glasgow outcome scale (GOS-E), the duration of postoperative ventilation, and intensive care unit (ICU) stay, mortality, Glasgow coma scale at discharge, and time to cranioplasty. We also evaluated and analyzed the impact of AC vs. DC on post-procedural intracranial pressure (ICP) and brain tissue oxygen (PbO2) values as well as the need for additional osmotherapy and CSF drainage.
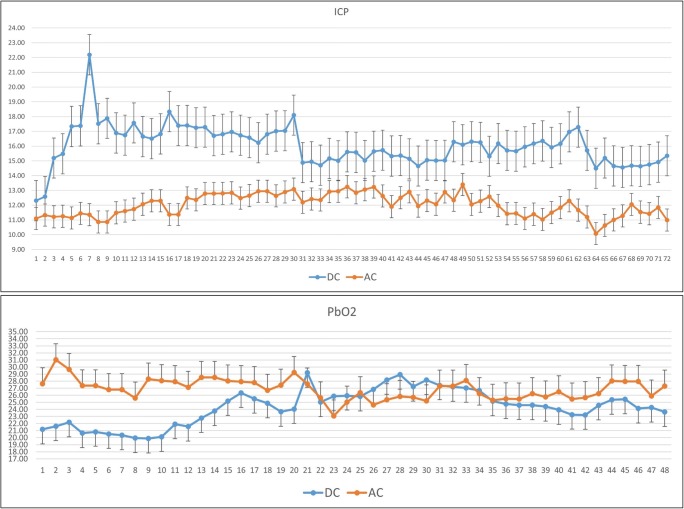
Results: Forty patients were examined, 22 patients in the DC group, and 18 in the AC group. Compared with DC alone, AC was associated with significant shorter duration of mechanical ventilation and ICU stay, as well as better Glasgow coma scale at discharge. Mortality rate was similar. At 6-month, the proportion of patients with favorable outcome (GOS-E ≥ 5) was higher in patients with AC vs. DC [10/18 patients (61%) vs. 7/20 (35%)]. The outcome difference was particularly relevant when AC was performed as primary procedure (61.5% vs. 18.2%; p = 0.04). Patients in the AC group also had significant lower average post-surgical ICP values, higher PbO2 values and required less osmotic treatments as compared with those treated with DC alone.
Conclusion: Our preliminary single-center retrospective data indicate that AC may be beneficial for the management of severe TBI and is associated with better clinical outcome. These promising results need further confirmation by larger multicenter clinical studies. The potential benefits of cisternostomy should not encourage its universal implementation across trauma care centers by surgeons that do not have the expertise and instrumentation necessary for cisternal microsurgery. Training in skull base and vascular surgery techniques for trauma care surgeons would avoid the potential complications associated with this delicate procedure.
Keywords: Cisternostomy; Decompressive craniectomy; Intracranial hypertension; Traumatic brain injury.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



Similar articles
-
Cisternostomy is not beneficial to reduce the occurrence of post-traumatic hydrocephalus in Traumatic Brain Injury.Acta Neurochir (Wien). 2024 Apr 30;166(1):200. doi: 10.1007/s00701-024-06084-0. Acta Neurochir (Wien). 2024. PMID: 38689141
-
Intracranial pressure monitoring after primary decompressive craniectomy in traumatic brain injury: a clinical study.Acta Neurochir (Wien). 2017 Apr;159(4):615-622. doi: 10.1007/s00701-017-3118-z. Epub 2017 Feb 24. Acta Neurochir (Wien). 2017. PMID: 28236181
-
Prognostic value of changes in brain tissue oxygen pressure before and after decompressive craniectomy following severe traumatic brain injury.J Neurosurg. 2018 May;128(5):1538-1546. doi: 10.3171/2017.1.JNS161840. Epub 2017 Jun 30. J Neurosurg. 2018. PMID: 28665250
-
Decompressive craniectomy for severe traumatic brain injury in children: analysis of long-term neuropsychological impairment and review of the literature.Childs Nerv Syst. 2019 Sep;35(9):1507-1515. doi: 10.1007/s00381-019-04274-1. Epub 2019 Jul 1. Childs Nerv Syst. 2019. PMID: 31264065 Review.
-
Early Decompressive Craniectomy as Management for Severe Traumatic Brain Injury in the Pediatric Population: A Comprehensive Literature Review.World Neurosurg. 2020 Jun;138:9-18. doi: 10.1016/j.wneu.2020.02.065. Epub 2020 Feb 19. World Neurosurg. 2020. PMID: 32084616 Review.
Cited by
-
Enhancing daily living and cognitive functions in traumatic brain injury patients through Orem's self-care theory.Front Neurol. 2024 Aug 20;15:1449417. doi: 10.3389/fneur.2024.1449417. eCollection 2024. Front Neurol. 2024. PMID: 39228512 Free PMC article.
-
Effect of Early Rehabilitation Nursing on Motor Function and Living Ability of Patients with Traumatic Brain Injury Based on Orem's Self-Care Theory.Comput Intell Neurosci. 2022 Sep 8;2022:7727085. doi: 10.1155/2022/7727085. eCollection 2022. Comput Intell Neurosci. 2022. PMID: 36120688 Free PMC article. Clinical Trial.
-
Basal Cisternostomy for Severe TBI: Surgical Technique and Cadaveric Dissection.Front Surg. 2022 May 6;9:915818. doi: 10.3389/fsurg.2022.915818. eCollection 2022. Front Surg. 2022. PMID: 35599786 Free PMC article.
-
Basal cisternostomy as an adjunct to decompressive hemicraniectomy in moderate to severe traumatic brain injury: a systematic review and meta-analysis.Neurosurg Rev. 2024 Oct 2;47(1):717. doi: 10.1007/s10143-024-02954-4. Neurosurg Rev. 2024. PMID: 39354191 Free PMC article.
-
Cisternostomy associated with decompressive craniectomy for traumatic brain injury: a systematic review and meta-analysis.Neurosurg Rev. 2024 Nov 15;47(1):850. doi: 10.1007/s10143-024-03102-8. Neurosurg Rev. 2024. PMID: 39542925
References
-
- Baucher Guillaume, Troude Lucas, Pauly Vanessa, Bernard Florian, Zieleskiewicz Laurent, Roche Pierre-Hugues. Predictive Factors of Poor Prognosis After Surgical Management of Traumatic Acute Subdural Hematomas: A Single-Center Series. World Neurosurgery. 2019;126:e944–e952. doi: 10.1016/j.wneu.2019.02.194. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
