

Metachronous rupture of a residual pancreaticoduodenal aneurysm after release of the median arcuate ligament: a case report
- PMID: 32016595
- PMCID: PMC6997311
- DOI: 10.1186/s40792-020-0784-5
Metachronous rupture of a residual pancreaticoduodenal aneurysm after release of the median arcuate ligament: a case report
Abstract
Background: Multiple pancreaticoduodenal artery aneurysms in association with median arcuate ligament syndrome (MALS) are relatively rare. A treatment option, such as a median arcuate ligament (MAL) release or embolization of the aneurysms, should be considered in such cases, but the treatment criteria remain unclear.
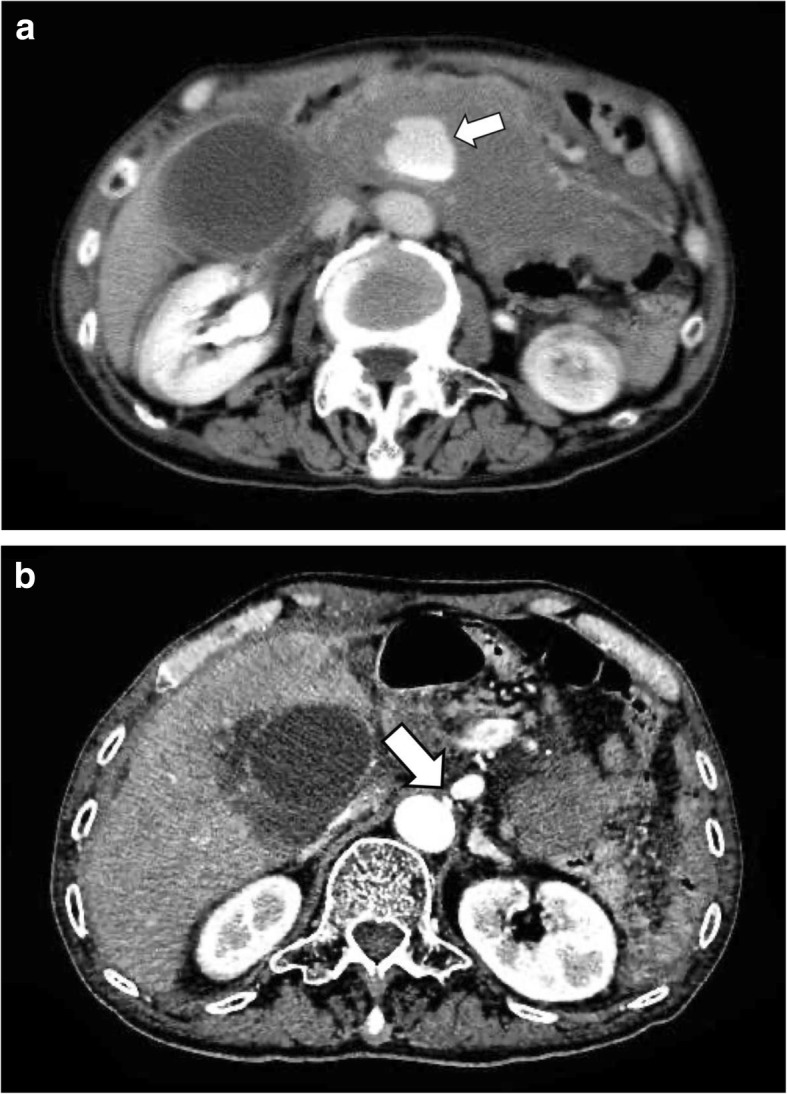
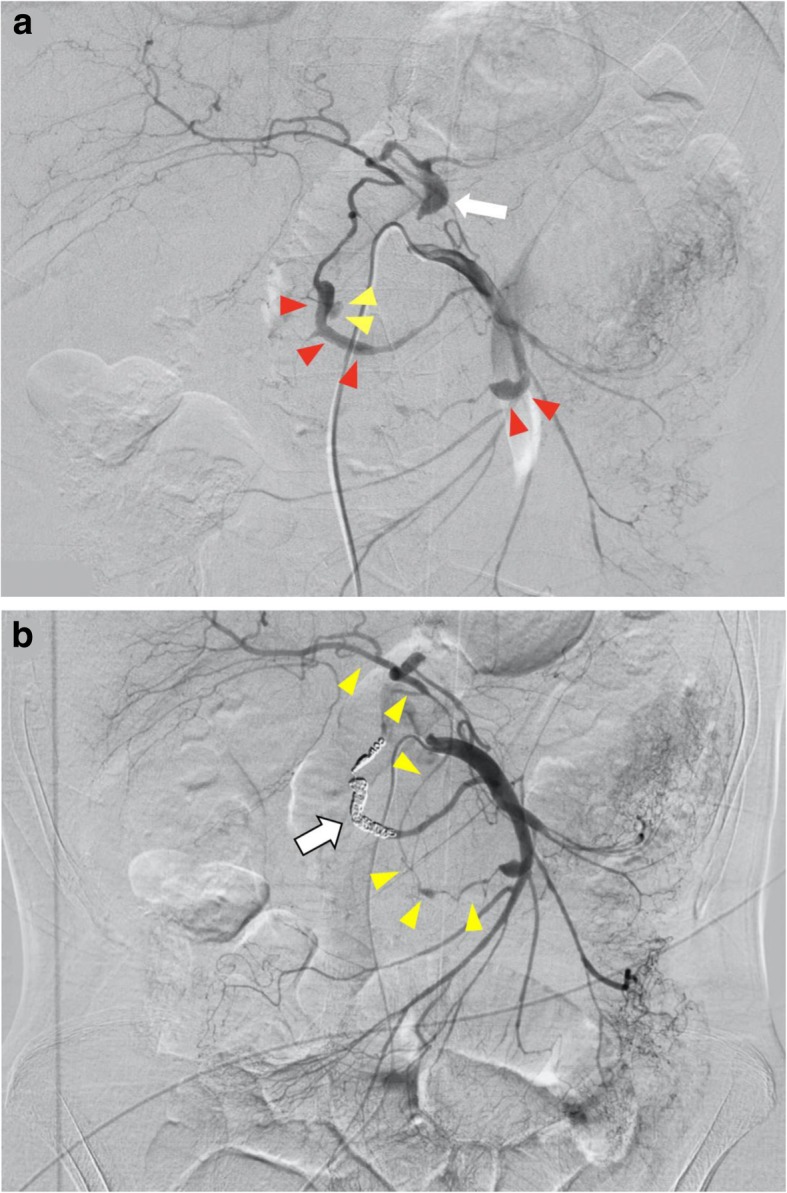
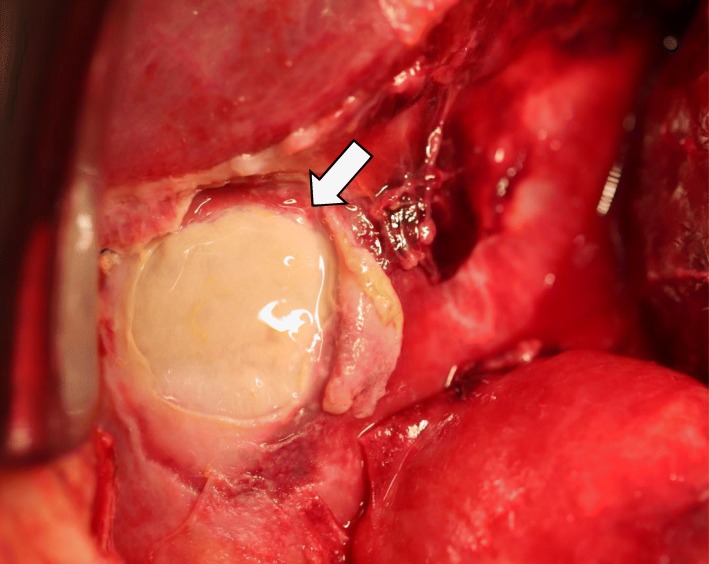
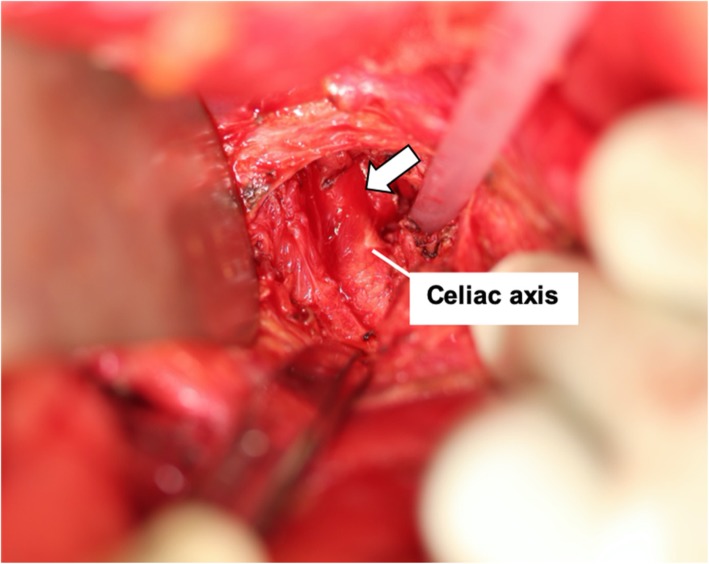
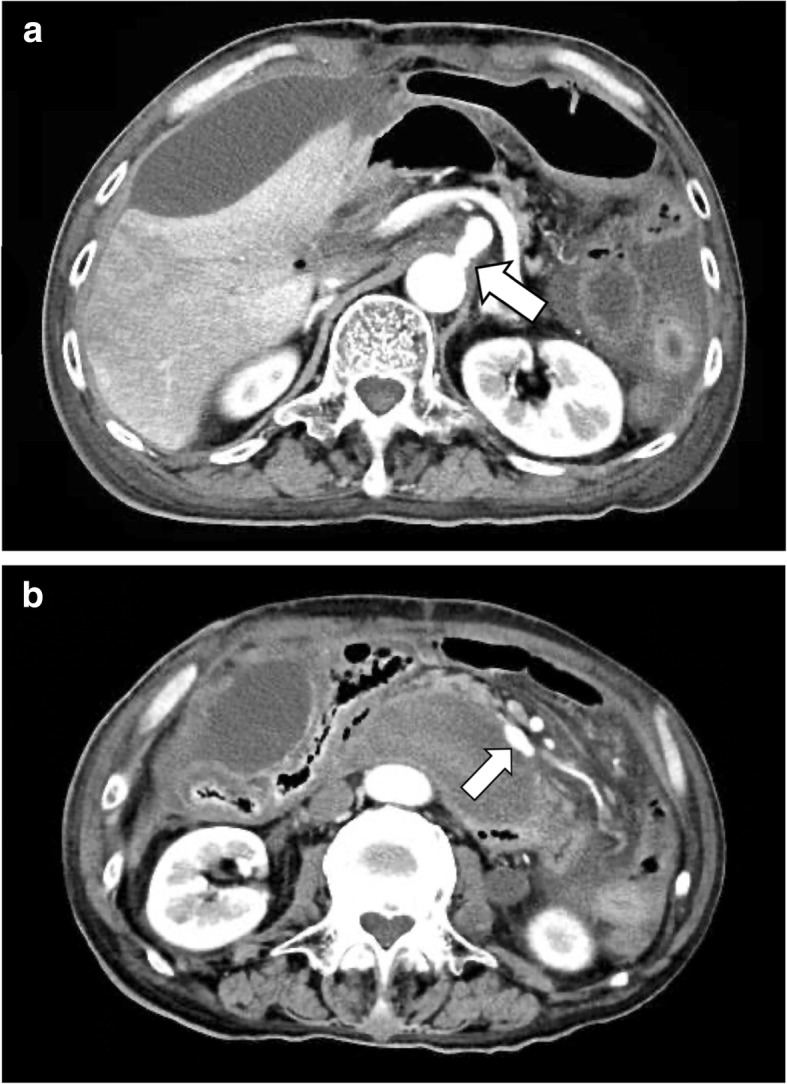
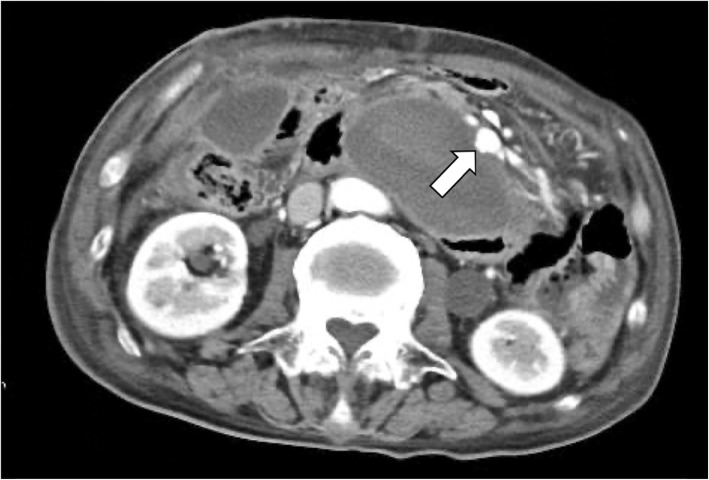
Case report: A 75-year-old man was transferred to our hospital because of a ruptured pancreaticoduodenal aneurysm. Emergency angiography showed stenosis of the root of the celiac axis (CA), a ruptured aneurysm of the posterior inferior pancreaticoduodenal artery (PIPDA), and an unruptured aneurysm of the anterior inferior pancreaticoduodenal artery (AIPDA). Coil embolization of the PIPDA was performed. Five days after embolization, the gallbladder became necrotic due to decreased blood flow in the CA region, and an emergency operation was performed. We performed a cholecystectomy and released the MAL to normalize the blood flow of the CA region. However, the patient died on postoperative day 8 because of rupture of the untreated aneurysm of the AIPDA.
Conclusions: This is the first report of metachronous ruptures of multiple pancreaticoduodenal aneurysms due to MALS, even after a MAL release. Although rare, a residual aneurysm in the pancreatic head region may need to be embolized quickly.
Keywords: Median arcuate ligament syndrome; Metachronous rupture; Multiple aneurysm; Segmental arterial mediolysis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Chivot C, Rebibo L, Robert B, Regimbeau JM, Yzet T. Ruptured pancreaticoduodenal artery aneurysms associated with celiac stenosis caused by the median arcuate ligament: a poorly known etiology of acute abdominal pain. Eur J Vasc Endovasc Surg. 2016;51(2):295–301. doi: 10.1016/j.ejvs.2015.10.025. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
