

Clinical Pharmacology and Safety of Trifarotene, a First-in-Class RARγ-Selective Topical Retinoid
- PMID: 32017149
- PMCID: PMC7187247
- DOI: 10.1002/jcph.1566
Clinical Pharmacology and Safety of Trifarotene, a First-in-Class RARγ-Selective Topical Retinoid
Abstract
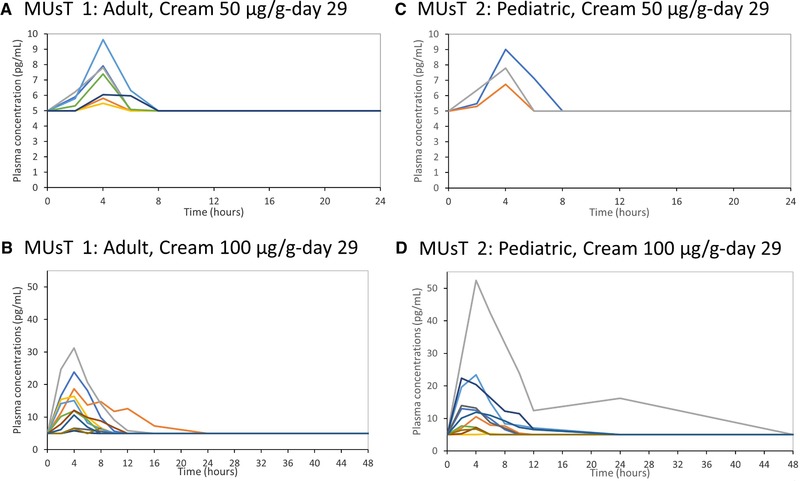
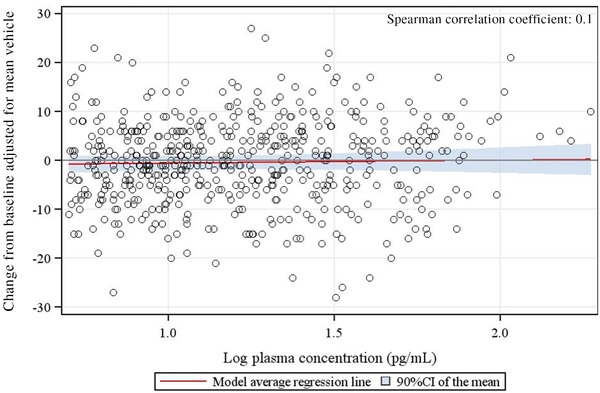
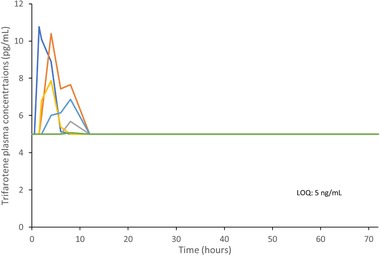
Trifarotene is a new drug with retinoic acid receptor activity and selectivity for retinoic acid receptor-γ. The reported studies aimed at assessing the clinical pharmacology and safety of trifarotene. The clinical pharmacology of topical trifarotene up to 100 µg/g was extensively investigated through 2 maximal usage pharmacokinetic trials (MUsT) conducted in adult (≥18 years) and pediatric patients (9-17 years) with moderate to severe acne and two studies conducted in healthy volunteers: 1 thorough QTC study and 1 drug-drug interaction study with concomitantly administered oral levonorgestrel (0.15 mg)/ethinyl estradiol (0.03 mg). Safety assessments included adverse event reporting and assessment of erythema, scaling, dryness, and stinging/burning using a scale from 0 = none to 4 = severe, as well as the evaluation of the systemic safety of trifarotene through routine laboratory testing. Systemic absorption of trifarotene was generally unquantifiable in the target population, especially when applied at 50 µg/g. QTC investigations did not show any risk of cardiovascular health issues; trifarotene did not reduce the systemic exposure to oral contraceptives such as levonorgestrel/ethinyl estradiol. Safety analyses did not show local or systemic safety concerns with trifarotene up 100 µg/g, a dose twice as high as the intended market dose. Results showed that trifarotene 50 µg/g cream is well tolerated and safe, even when applied under maximized conditions in adults and pediatric acne patients presenting with severe acne. Daily use of trifarotene 50 µg/g cream was not associated with cardiovascular effects and did not result in drug-drug interaction in women of childbearing potential using oral contraception.
Keywords: MUsT; TQC study; drug-drug interaction; pharmacokinetics; trifarotene.
© 2020 Galderma. The Journal of Clinical Pharmacology published by Wiley Periodicals, Inc. on behalf of American College of Clinical Pharmacology.
Conflict of interest statement
N.W., A.A.S., and M.G. are employees of Galderma R&D, LLC. USA. K.B. and M.P. were employees of Galderma R&D, France, at the time the studies were conducted. V.S. from Sanders Medical Writing and K.P.G., SMWS France, have no conflicts of interest to disclose
Figures

References
-
- Oudenhoven MD, Kinney MA, McShane DB, Burkhart CN, Morrell DS. Adverse effects of acne medications: recognition and management. Am J Clin Dermatol. 2015;16(4):231‐242. - PubMed
-
- Dreno B. What is new in the pathophysiology of acne, an overview. J Eur Acad Dermatol Venereol. 2017;31(suppl 5):8‐12. - PubMed
-
- Eichenfield LF, Krakowski AC, Piggott C, et al. Evidence‐based recommendations for the diagnosis and treatment of pediatric acne. Pediatrics. 2013;131(suppl 3):S163‐S186. - PubMed
-
- Aubert J, Piwnica D, Bertino B, et al. Nonclinical and human pharmacology of the potent and selective topical retinoic acid receptor‐gamma agonist trifarotene. Br J Dermatol. 2018;179(2):442‐456. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
