

Utility of low-dose gelatin sponge particles and 5% ethanolamine oleate iopamidol mixture in retrograde transvenous obliteration (GERTO) for gastric varices
- PMID: 32017608
- PMCID: PMC7362928
- DOI: 10.1259/bjr.20190751
Utility of low-dose gelatin sponge particles and 5% ethanolamine oleate iopamidol mixture in retrograde transvenous obliteration (GERTO) for gastric varices
Abstract
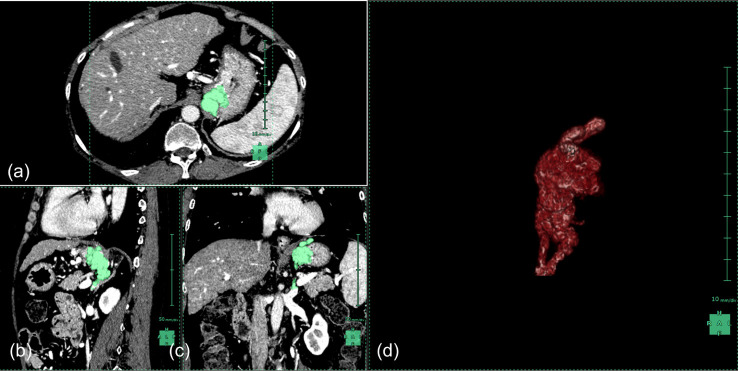
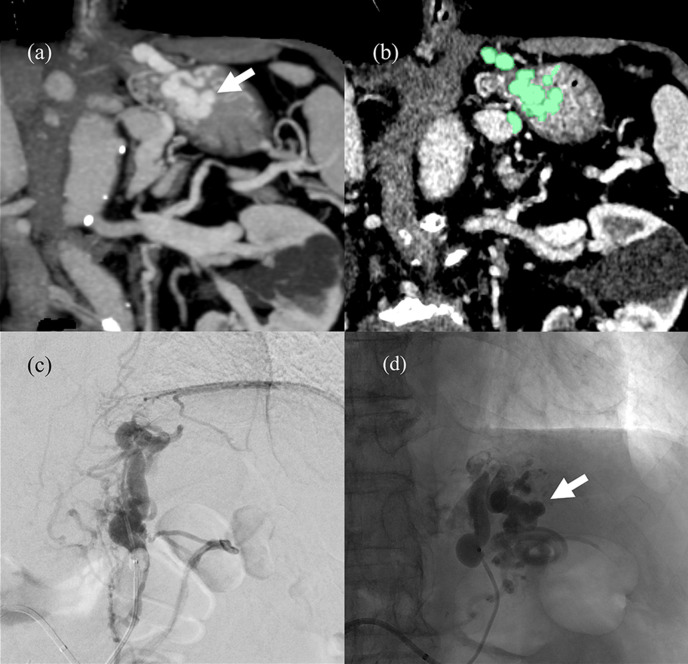
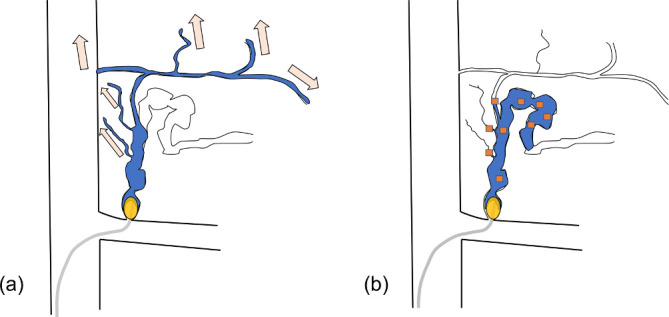
Objective: To determine the utility of low-dose gelatin sponge particles and 5% ethanolamine oleate iopamidol (EOI) mixture in retrograde transvenous obliteration (GERTO) for gastric varices (GV).
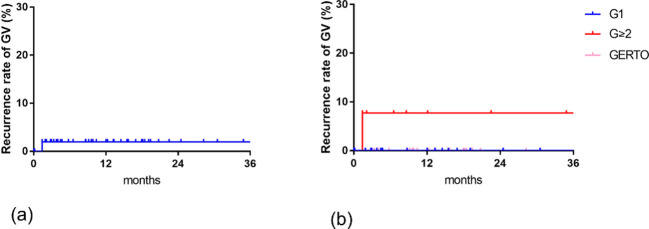
Methods: 57 consecutive patients who underwent balloon-occluded retrograde transvenous obliteration (B-RTO) for GV were divided into three groups with Hirota's grade by balloon-occluded retrograde transvenous venography. Hirota's Grade 1 patients were assigned to G1 group and underwent treatment with 5% EOI. Grade ≥ 2 patients prior to August 2015 were G ≥ 2 group treated with 5% EOI, and those treated thereafter were GERTO group. The amount of EOI used per unit GV volume (EOI/GV ratio), the times to embolization and recurrence rate of GV were evaluated.
Results: The EOI/GV ratio was 0.66 ± 0.19 in G1, 1.5 ± 0.8 in G ≥ 2, and 0.58 ± 0.23 in GERTO (G ≥ 2 vs GERTO, p < 0.0001). The times to embolization were 26.5 ± 10.5 min for G1, 39.2 ± 26.8 for G ≥ 2, and 21.4 ± 9.4 for GERTO (G ≥ 2 vs GERTO, p = 0.005). The recurrence rate was not significantly different in any of the groups.
Conclusion: GERTO was performed in lower amount of sclerosants and in less time compared to conventional B-RTO in Hirota's grade ≥2.
Advances in knowledge: Feasibility of low-dose gelatin sponge particles and 5% EOI mixture as sclerosants for GV.
Figures
References
-
- Trolle E, Trolle D. Treatment of oesophageal varices by injections of sclerosing agents through oesophagoscope in splenectomized patient suffering from splenic phlebostenosis (splenic anemia); a case with autopsy. Acta Chir Scand 1946; 94: 385–96. - PubMed
