

Clinical characteristics, CT signs, and pathological findings of Pyrrolizidine alkaloids-induced sinusoidal obstructive syndrome: a retrospective study
- PMID: 32019495
- PMCID: PMC7001201
- DOI: 10.1186/s12876-020-1180-0
Clinical characteristics, CT signs, and pathological findings of Pyrrolizidine alkaloids-induced sinusoidal obstructive syndrome: a retrospective study
Abstract
Background: One major etiology of hepatic sinusoidal obstruction syndrome (HSOS) in China is the intake of pyrrolizidine alkaloids (PAs). Since PAs-induced HSOS is a rare disease that has not been clearly characterized until now, the aim of this study was to investigate clinical characteristics, CT features, and pathological findings of PA-induced HSOS.
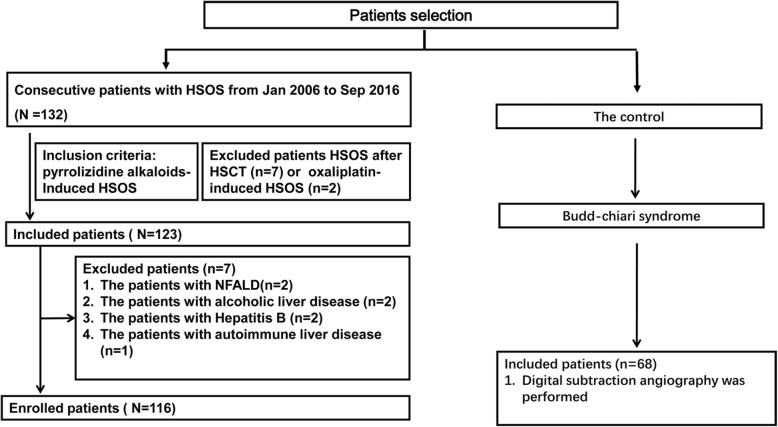
Methods: This retrospective cohort study included 116 patients with PAs-induced HSOS and 68 patients with Budd-Chiari syndrome from Jan 2006 to Sep 2016. We collected medical records of the patients, and reviewed image features of CT, and analyzed pathological findings.
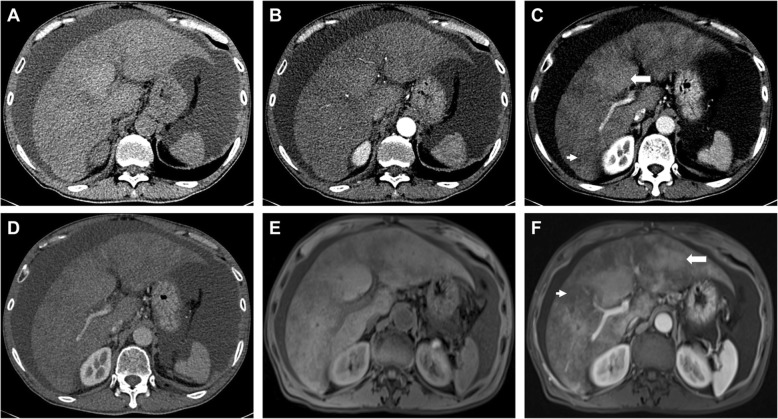
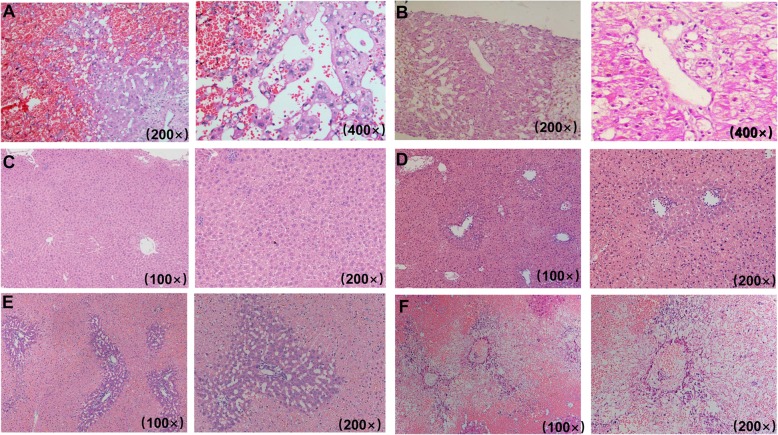
Results: Common clinical manifestations of PAs-induced HSOS were abdominal distention (98.26%), ascites (100%), jaundice (52.94%), abdominal pain (36.36%). Abnormal liver function was observed in most of PAs-induced HSOS. On CT scan, common findings included: ascites, hepatomegaly, the thickening of gallbladder wall, pleural effusion, patchy liver enhancement, and heterogeneous hypoattenuation. Most of the patients had a low ascitic total protein (< 25 g/L) and a high SAAG (≥ 11.0 g/L). In acute stage, pathologic features were massive sinusoidal dilatation, sinusoidal congestion, the extravasation of erythrocytes, hepatocellular necrosis, the accumulation of macrophages, the deposition of hemosiderin. In subacute stage, complete loss of pericentral hepatocytes, sinusoidal dilatation, the deposition of pigment granules were observed.
Conclusions: The PAs-induced HSOS patients displayed distinct clinical characteristics, imaging features, and pathological findings, which provided some evidences for the diagnosis of PAs-induced HSOS.
Trial registration: ChiCTR-DRD-17010709.
Keywords: Ascites; Clinical manifestations; Hepatic sinusoidal obstruction syndrome; Histology; Pyrrolizidine alkaloid.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Diagnostic performance of Contrast-enhanced CT in Pyrrolizidine Alkaloids-induced Hepatic Sinusoidal Obstructive Syndrome.Sci Rep. 2016 Nov 29;6:37998. doi: 10.1038/srep37998. Sci Rep. 2016. PMID: 27897243 Free PMC article.
-
Pyrrolizidine alkaloids-induced hepatic sinusoidal obstruction syndrome: Pathogenesis, clinical manifestations, diagnosis, treatment, and outcomes.World J Gastroenterol. 2019 Jul 28;25(28):3753-3763. doi: 10.3748/wjg.v25.i28.3753. World J Gastroenterol. 2019. PMID: 31391770 Free PMC article. Review.
-
Definitive diagnosis of hepatic sinusoidal obstruction syndrome induced by pyrrolizidine alkaloids.J Dig Dis. 2012 Jan;13(1):33-9. doi: 10.1111/j.1751-2980.2011.00552.x. J Dig Dis. 2012. PMID: 22188914
-
Gadoxetic Acid-Enhanced Hepatobiliary-Phase Magnetic Resonance Imaging for Pyrrolizidine Alkaloid-Induced Hepatic Sinusoidal Obstruction Syndrome and Association with Liver Function.Sci Rep. 2019 Feb 4;9(1):1231. doi: 10.1038/s41598-018-37775-1. Sci Rep. 2019. PMID: 30718698 Free PMC article.
-
Expert consensus on the clinical management of pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome.J Gastroenterol Hepatol. 2019 Apr;34(4):634-642. doi: 10.1111/jgh.14612. Epub 2019 Feb 21. J Gastroenterol Hepatol. 2019. PMID: 30669184 Review.
Cited by
-
Difference between type 2 gastroesophageal varices and isolated fundic varices in clinical profiles and portosystemic collaterals.World J Clin Cases. 2022 Jun 16;10(17):5620-5633. doi: 10.12998/wjcc.v10.i17.5620. World J Clin Cases. 2022. PMID: 35979133 Free PMC article.
-
Drug-induced hepatic sinusoidal obstruction syndrome: current advances and future perspectives.Arch Toxicol. 2025 Mar;99(3):835-850. doi: 10.1007/s00204-024-03950-9. Epub 2024 Dec 24. Arch Toxicol. 2025. PMID: 39718593 Review.
-
Development of a Drum Tower Severity Scoring (DTSS) system for pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome.Hepatol Int. 2022 Jun;16(3):669-679. doi: 10.1007/s12072-021-10293-5. Epub 2022 Jan 12. Hepatol Int. 2022. PMID: 35023026 Free PMC article. Clinical Trial.
-
Radical total gastrectomy for gastric cancer complicated by hepatic sinusoidal obstruction syndrome: a case report.Front Med (Lausanne). 2025 May 9;12:1544400. doi: 10.3389/fmed.2025.1544400. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40417670 Free PMC article.
-
Prognostic factors for pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome: a multicenter study in China.Ann Transl Med. 2021 Jan;9(1):11. doi: 10.21037/atm-20-731. Ann Transl Med. 2021. PMID: 33553304 Free PMC article.
References
-
- Blostein MD, Paltiel OB, Thibault A, Rybka WB. A comparison of clinical criteria for the diagnosis of veno-occlusive disease of the liver after bone marrow transplantation. Bone Marrow Transplant. 1992;10(5):439–443. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
