

Tumor Mutational Burden and PTEN Alterations as Molecular Correlates of Response to PD-1/L1 Blockade in Metastatic Triple-Negative Breast Cancer
- PMID: 32019858
- PMCID: PMC7269810
- DOI: 10.1158/1078-0432.CCR-19-3507
Tumor Mutational Burden and PTEN Alterations as Molecular Correlates of Response to PD-1/L1 Blockade in Metastatic Triple-Negative Breast Cancer
Abstract
Purpose: Few patients with metastatic triple-negative breast cancer (mTNBC) benefit from immune checkpoint inhibitors (ICI). On the basis of immunotherapy response correlates in other cancers, we evaluated whether high tumor mutational burden (TMB) ≥10 nonsynonymous mutations/megabase and PTEN alterations, defined as nonsynonymous mutations or 1 or 2 copy deletions, were associated with clinical benefit to anti-PD-1/L1 therapy in mTNBC.
Experimental design: We identified patients with mTNBC, who consented to targeted DNA sequencing and were treated with ICIs on clinical trials between April 2014 and January 2019 at Dana-Farber Cancer Institute (Boston, MA). Objective response rate (ORR), progression-free survival (PFS), and overall survival (OS) were correlated with tumor genomic features.
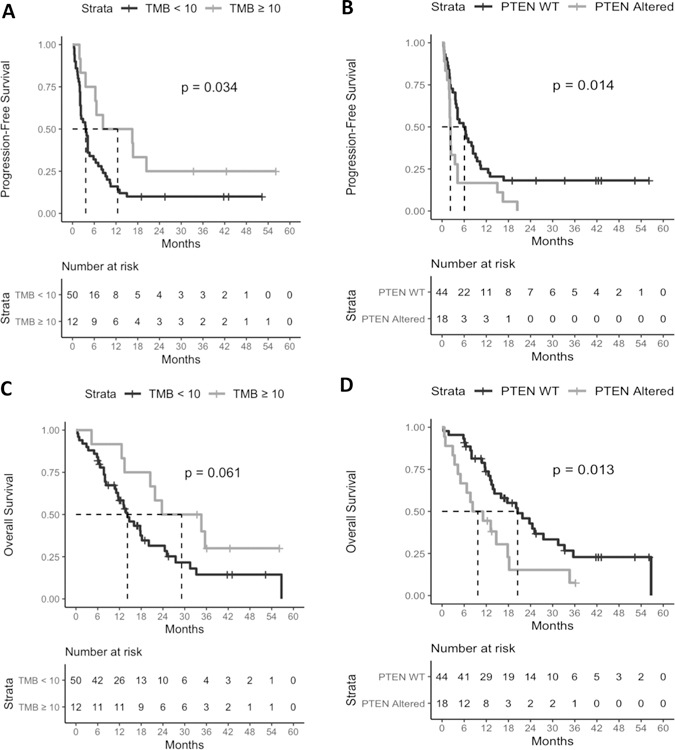
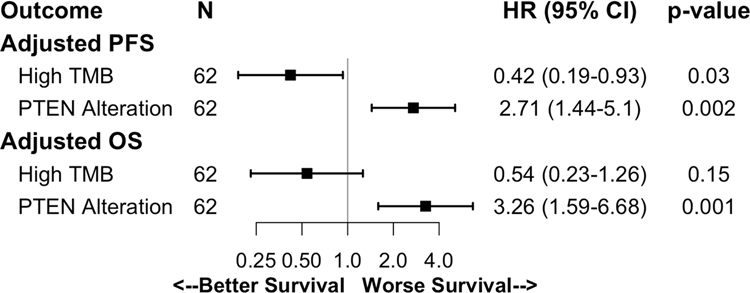
Results: Sixty-two women received anti-PD-1/L1 inhibitors alone (23%) or combined with targeted therapy (19%) or chemotherapy (58%). High TMB (18%) was associated with significantly longer PFS (12.5 vs. 3.7 months; P = 0.04), while PTEN alterations (29%) were associated with significantly lower ORR (6% vs. 48%; P = 0.01), shorter PFS (2.3 vs. 6.1 months; P = 0.01), and shorter OS (9.7 vs. 20.5 months; P = 0.02). Multivariate analyses confirmed that these associations were independent of performance status, prior lines of therapy, therapy regimen, and visceral metastases. The survival associations were additionally independent of PD-L1 in patients with known PD-L1 and were not found in mTNBC cohorts treated with chemotherapy (n = 90) and non-ICI regimens (n = 169).
Conclusions: Among patients with mTNBC treated with anti-PD-1/L1 therapies, high TMB and PTEN alterations were associated with longer and shorter survival, respectively. These observations warrant validation in larger datasets.
©2020 American Association for Cancer Research.
Figures
References
-
- Adams S, Loi S, Toppmeyer D, Cescon DW, De Laurentiis M, Nanda R, et al. Phase 2 study of pembrolizumab as first-line therapy for PD-L1–positive metastatic triple-negative breast cancer (mTNBC): Preliminary data from KEYNOTE-086 cohort B. J Clin Oncol 2017;35:1088–1088.
-
- Adams S, Schmid P, Rugo HS, Winer EP, Loirat D, Awada A, et al. Phase 2 study of pembrolizumab (pembro) monotherapy for previously treated metastatic triple-negative breast cancer (mTNBC): KEYNOTE-086 cohort A. J Clin Oncol 2017;35:Abstr 1008. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
