

CEUS LI-RADS: a pictorial review
- PMID: 32020352
- PMCID: PMC7000618
- DOI: 10.1186/s13244-019-0819-2
CEUS LI-RADS: a pictorial review
Abstract
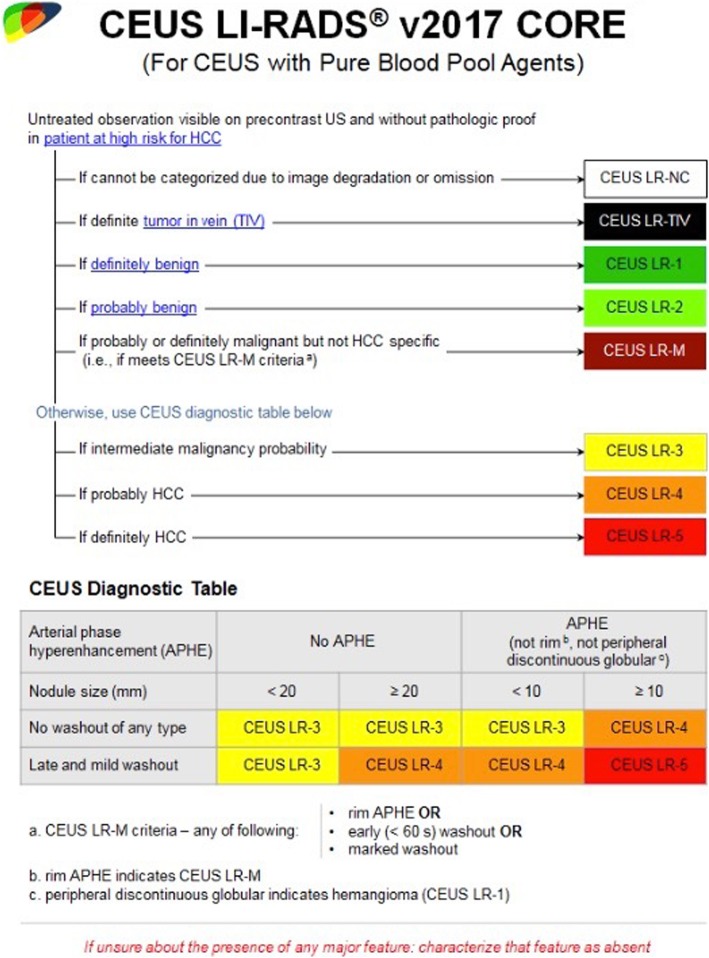
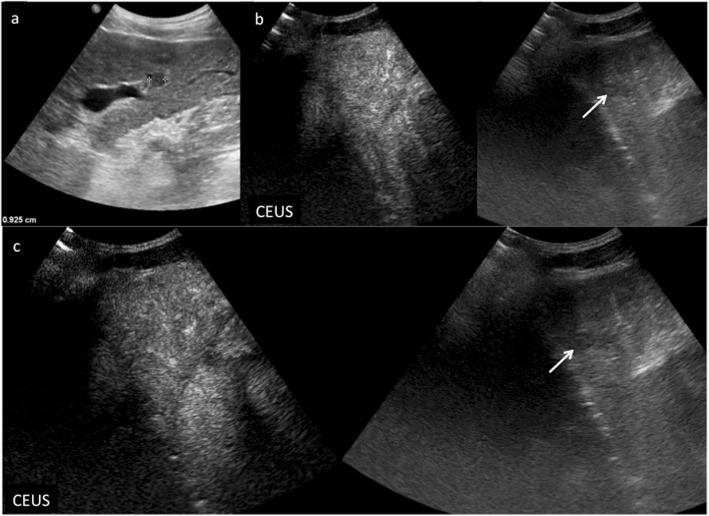
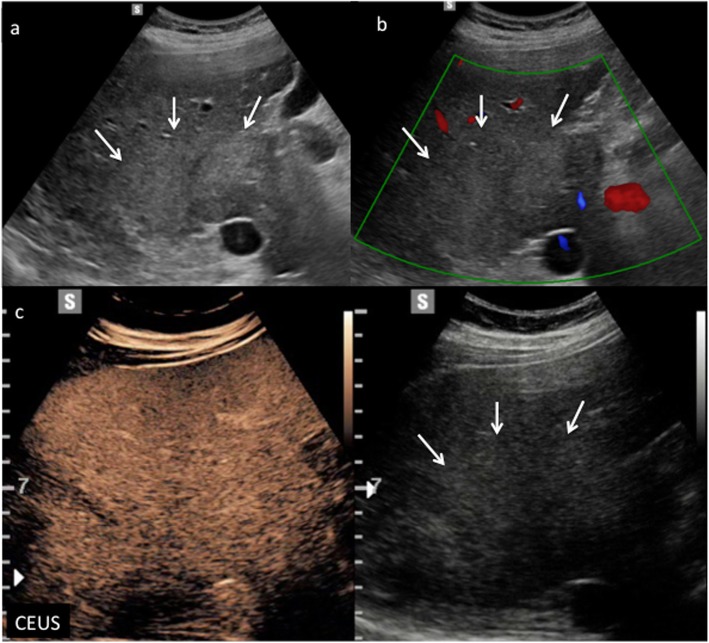
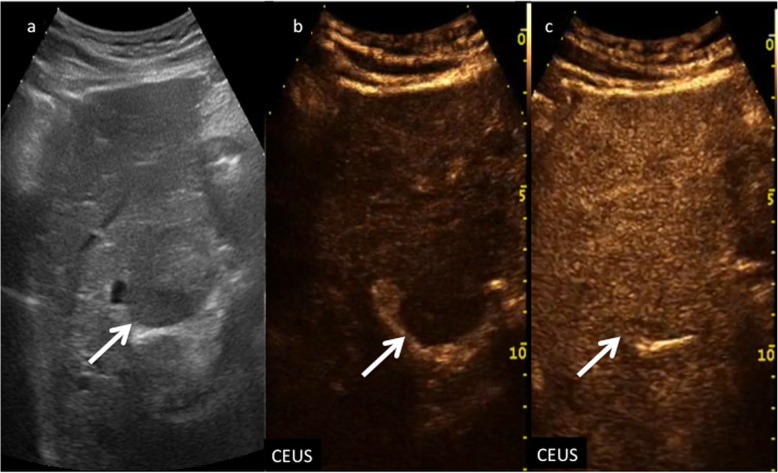
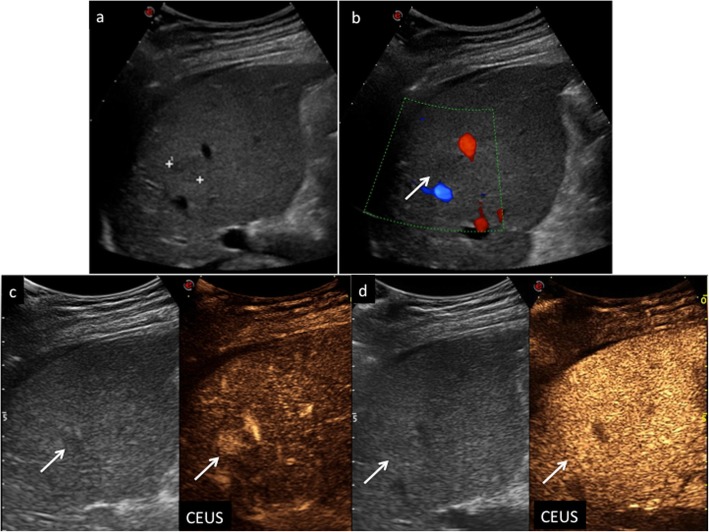
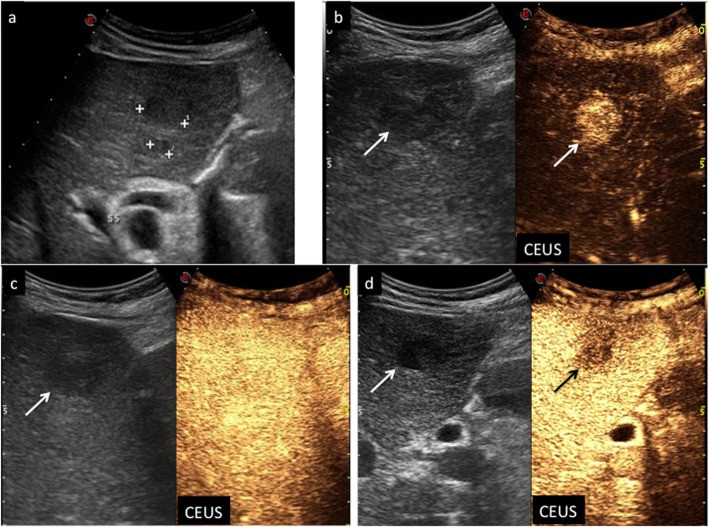
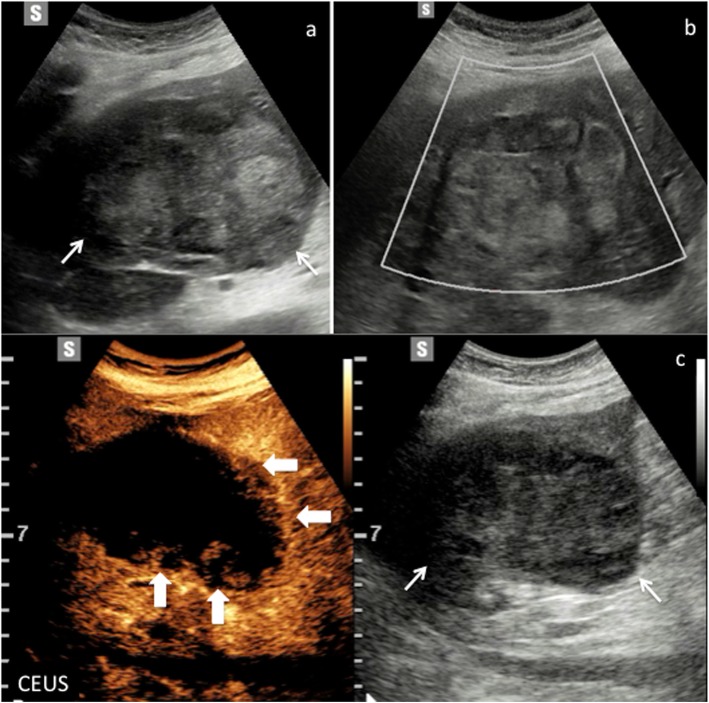
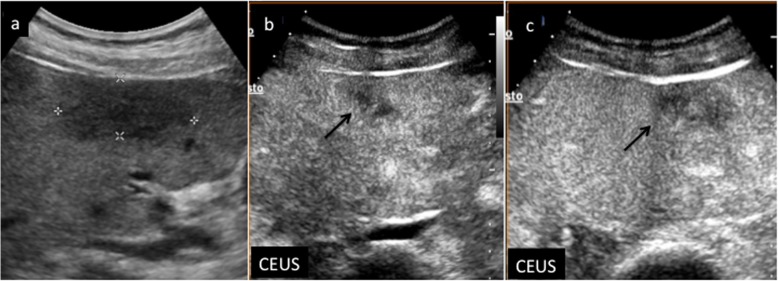
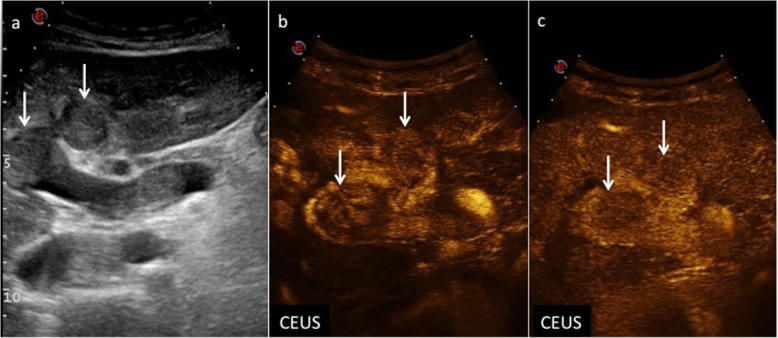
Contrast-enhanced ultrasound (CEUS) greatly improved the diagnostic accuracy of US in the detection and characterization of focal liver lesions (FLLs), and it is suggested and often included in many international guidelines as an important diagnostic tool in the imaging work-up of cirrhotic patients at risk for developing hepatocellular carcinoma (HCC). In particular, CEUS Liver Imaging Reporting and Data System (LI-RADS) provides standardized terminology, interpretation, and reporting for the diagnosis of HCC. The aim of this pictorial essay is to illustrate CEUS features of nodules discovered at US in cirrhotic liver according to LI-RADS categorization.
Keywords: Cholangiocarcinoma; Cirrhosis; Contrast-enhanced ultrasonography; Hepatocellular carcinoma; Liver tumor characterization.
Conflict of interest statement
One author (TVB) is a scientific advisor for Samsung.
Figures
References
-
- World Health organization, International Agency for Research on Cancer, Global Cancer Observatory Cancer Today – IARC, Lyon, France, 2018 available via http://gco.iarc.fr/today/data/factsheets/cancers/11-Liver-fact-sheet.pdf. Last accessed 8 Jan 2019
-
- European Association for the Study of the Liver (2018) EASL clinical practice guidelines: management of hepatocellular carcinoma. European Association for the Study of the Liver. J Hepatol 69(1):182–236 - PubMed
-
- Omata Masao, Cheng Ann-Lii, Kokudo Norihiro, Kudo Masatoshi, Lee Jeong Min, Jia Jidong, Tateishi Ryosuke, Han Kwang-Hyub, Chawla Yoghesh K., Shiina Shuichiro, Jafri Wasim, Payawal Diana Alcantara, Ohki Takamasa, Ogasawara Sadahisa, Chen Pei-Jer, Lesmana Cosmas Rinaldi A., Lesmana Laurentius A., Gani Rino A., Obi Shuntaro, Dokmeci A. Kadir, Sarin Shiv Kumar. Asia–Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatology International. 2017;11(4):317–370. doi: 10.1007/s12072-017-9799-9. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
