

Annual Research Review: Defining and treating pediatric treatment-resistant depression
- PMID: 32020643
- PMCID: PMC8314167
- DOI: 10.1111/jcpp.13202
Annual Research Review: Defining and treating pediatric treatment-resistant depression
Abstract
Background: Adolescent major depressive disorder (MDD) is a significant health problem, associated with substantial morbidity, cost, and mortality. Depression is a significant risk factor for suicide, which is now the second leading cause of death in young people. Up to twenty per cent of adolescents will experience MDD before adulthood, and while a substantial proportion will improve with standard-of-care treatments (psychotherapy and medication), roughly one third will not.
Methods: Here, we have reviewed the literature in order to discuss the concept of treatment-resistant depression (TRD) in adolescence, examine risk factors, diagnostic difficulties, and challenges in evaluating symptom improvement, and providing guidance on how to define adequate medication and psychotherapy treatment trials.
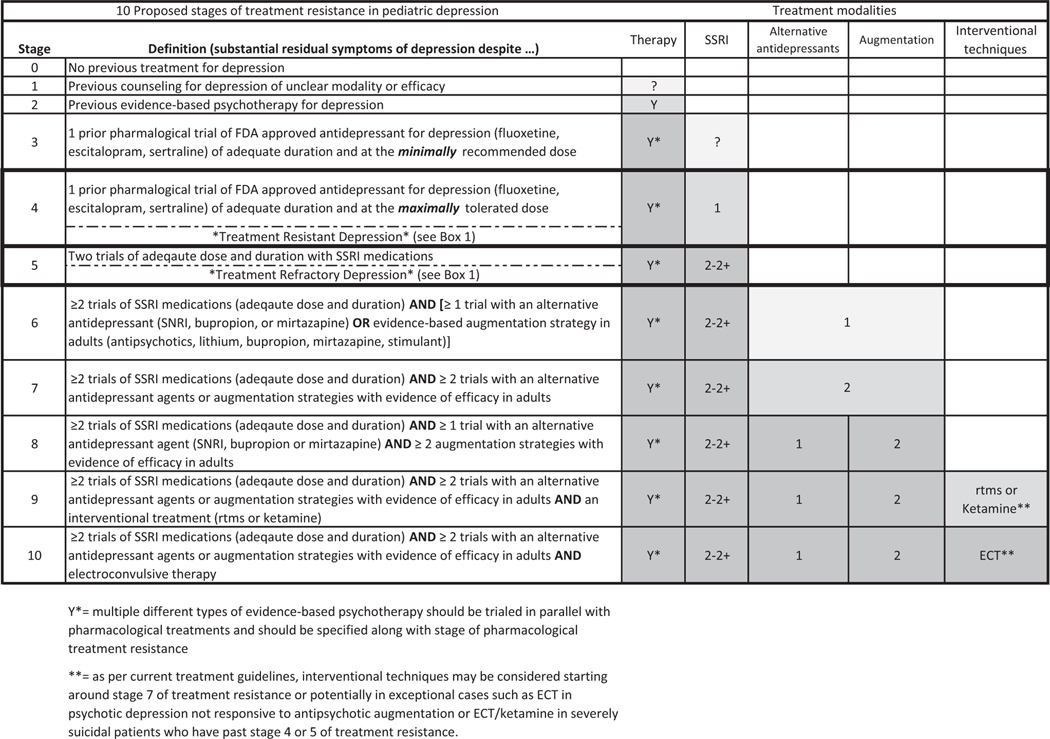
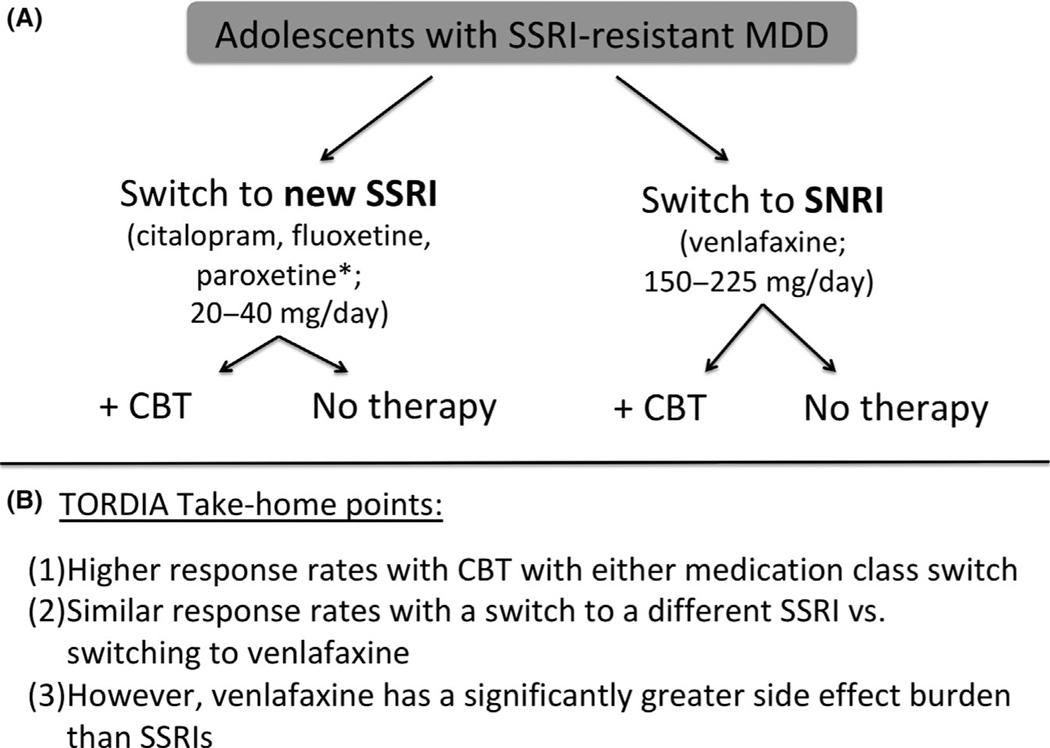
Results: We propose a staging model for adolescent TRD and review the treatment literature. The evidence base for first- and second-line treatments primarily derives from four large pediatric clinical trials (TADS, TORDIA, ADAPT, and IMPACT). After two medications and a trial of evidence-based psychotherapy have failed to alleviate depressive symptoms, the evidence becomes quite thin for subsequent treatments. Here, we review the evidence for the effectiveness of medication switches, medication augmentation, psychotherapy augmentation, and interventional treatments (i.e., transcranial magnetic stimulation, electroconvulsive therapy, and ketamine) for adolescent TRD. Comparisons are drawn to the adult TRD literature, and areas for future pediatric depression research are highlighted.
Conclusions: As evidence is limited for treatments in this population, a careful consideration of the known risks and side effects of escalated treatments (e.g., mood stabilizers and atypical antipsychotics) is warranted and weighed against potential, but often untested, benefits.
Keywords: Depression; major depressive disorder; psychopharmacology; psychotherapy.
© 2020 Association for Child and Adolescent Mental Health.
Conflict of interest statement
Conflict of interest statement: See Acknowledgements for full disclosures.
Figures
Comment in
-
Commentary: Treatment failure and success: a commentary on defining and treating pediatric treatment-resistant depression - reflections on Dwyer et al. (2020).J Child Psychol Psychiatry. 2020 Mar;61(3):333-335. doi: 10.1111/jcpp.13207. Epub 2020 Feb 7. J Child Psychol Psychiatry. 2020. PMID: 32034765 Free PMC article.
References
-
- Almeida OP, Ford AH, & Flicker L. (2015). Systematic review and meta-analysis of randomized placebo-controlled trials of folate and vitamin B12 for depression. International Psychogeriatrics, 27, 727–737. - PubMed
-
- APA (2013). Diagnostic and statistical manual of mental disorders (5th edn). Arlington, VA: Author.
-
- Atkinson SD, Prakash A, Zhang Q, Pangallo BA, Bangs ME, Emslie GJ, & March JS (2014). A double-blind efficacy and safety study of duloxetine flexible dosing in children and adolescents with major depressive disorder. Journal of Child and Adolescent Psychopharmacology, 24, 180–189. - PubMed
-
- Axelson DA, Perel JM, Birmaher B, Rudolph GR, Nuss S, Bridge J, & Brent DA (2002). Sertraline pharmacokinetics and dynamics in adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 1037–1044. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
