

Comparison of Biologics and Oral Treatments for Plaque Psoriasis: A Meta-analysis
- PMID: 32022825
- PMCID: PMC7042876
- DOI: 10.1001/jamadermatol.2019.4029
Comparison of Biologics and Oral Treatments for Plaque Psoriasis: A Meta-analysis
Abstract
Importance: The clinical benefits of novel treatments for moderate to severe psoriasis are well established, but wide variations exist in patient response across different therapies. In the absence of head-to-head randomized trials, meta-analyses synthesizing data from multiple studies are needed to assess comparative efficacy among psoriasis treatments.
Objective: To estimate the relative short-term and long-term efficacy of biologics and oral agents for the treatment of moderate to severe psoriasis.
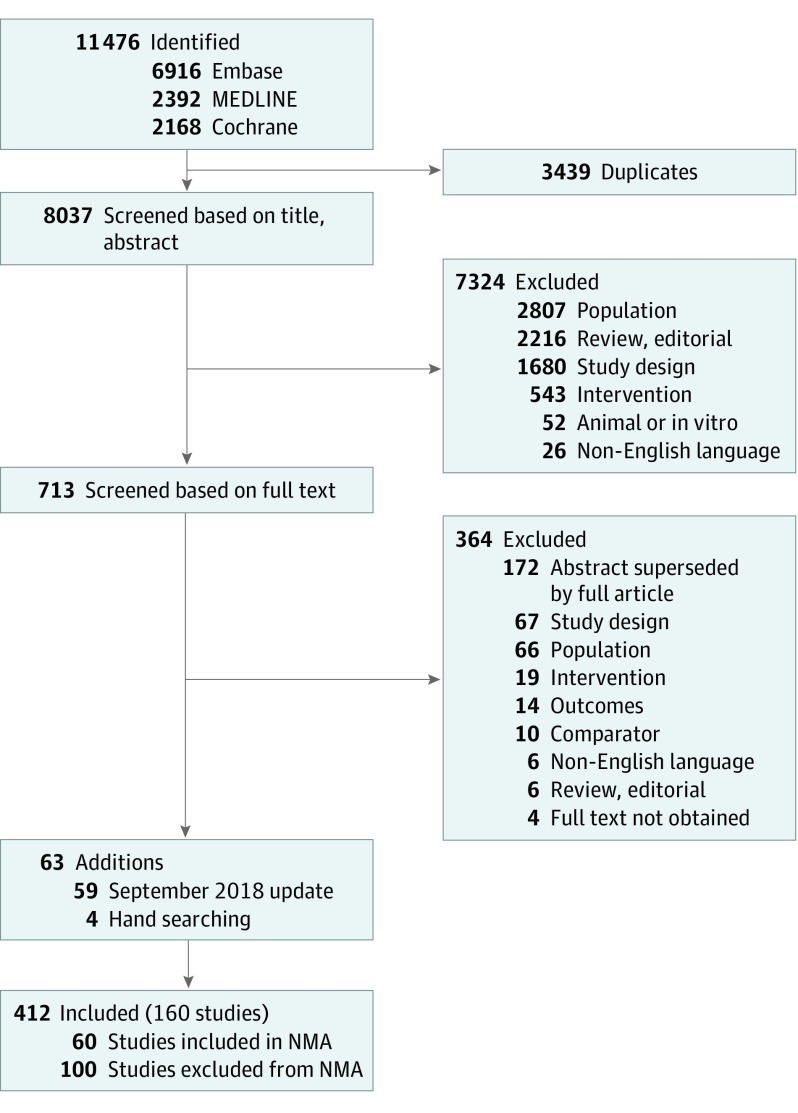
Data sources: A systematic literature review was conducted on December 4, 2017, and updated on September 17, 2018. The Embase, MEDLINE, and Cochrane Central Register databases were included.
Study selection: Phase 2, 3, or 4 randomized clinical trials of treatments licensed by the US Food and Drug Administration and the European Medicines Agency for adults with moderate to severe psoriasis with data on Psoriasis Area and Severity Index assessment of 75%, 90%, and 100% reductions (PASI 75, 90, and 100) at 10 to 16 weeks (short-term efficacy) or 44 to 60 weeks (long-term efficacy) from baseline.
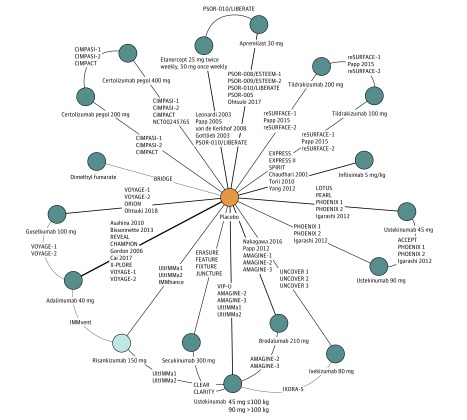
Data extraction and synthesis: Data were extracted based on the Preferred Reporting Items for Systematic Review and Meta-analysis guidelines. A bayesian network meta-analysis was conducted to estimate short-term PASI response rates; to account for variation across trials, an ordinal model that adjusted for reference arm response was implemented. The long-term PASI rates were estimated via a traditional meta-analysis.
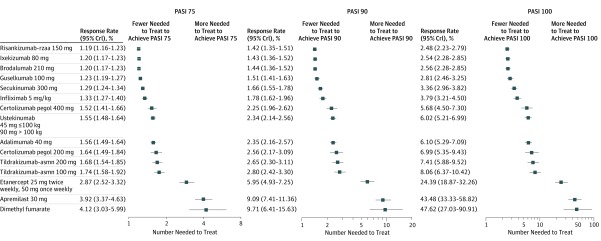
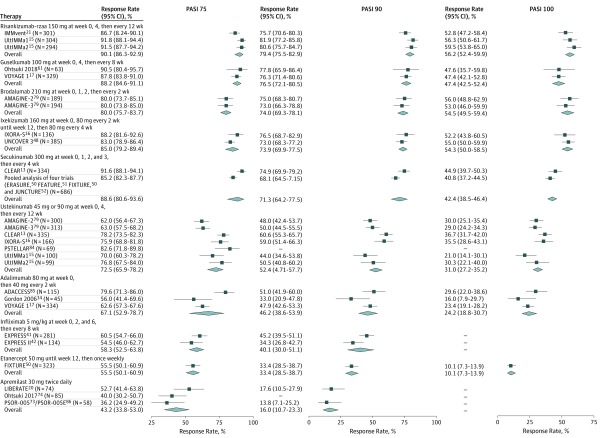
Main outcomes and measures: PASI 75, 90, and 100 response rates at 10 to 16 weeks and 44 to 60 weeks from baseline.
Results: Sixty trials meeting all inclusion criteria were included. At weeks 10 to 16, the highest PASI 90 rates were seen with risankizumab-rzaa (71.6%; 95% credible interval [CrI], 67.5%-75.4%), brodalumab (70.8%; 95% CrI, 66.8%-74.6%), ixekizumab (70.6%; 95% CrI, 66.8%-74.6%), and guselkumab (67.3%; 62.5%-71.9%). At weeks 44 to 60, the treatments with the highest PASI 90 rates were risankizumab-rzaa (79.4%, 95% CI, 75.5%-82.9%), guselkumab (76.5%; 95% CI, 72.1%-80.5%), brodalumab (74.0%; 95% CI, 69.3%-78.1%), and ixekizumab (73.9%; 95% CI, 69.9%-77.5%). Findings were consistent for short-term and long-term PASI 75 and 100 responses.
Conclusions and relevance: This study provides an assessment of the comparative efficacy among treatments for moderate to severe plaque psoriasis. The meta-analysis suggests that brodalumab, guselkumab, ixekizumab, and risankizumab-rzaa were associated with the highest PASI response rates in both short-term and long-term therapy.
Conflict of interest statement
Figures
Comment in
-
Comparative Effectiveness Studies for Psoriasis-The Methods Matter.JAMA Dermatol. 2020 Mar 1;156(3):253-255. doi: 10.1001/jamadermatol.2019.4025. JAMA Dermatol. 2020. PMID: 32022830 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
