

Separating the effects of 24-hour urinary chloride and sodium excretion on blood pressure and risk of hypertension: Results from PREVEND
- PMID: 32023312
- PMCID: PMC7001936
- DOI: 10.1371/journal.pone.0228490
Separating the effects of 24-hour urinary chloride and sodium excretion on blood pressure and risk of hypertension: Results from PREVEND
Abstract
Objective: Research into dietary factors associated with hypertension has focused on the sodium component of salt. However, chloride has distinct physiological effects that may surpass the effect of sodium on blood pressure. This study aims to separate the specific effects of chloride and sodium intake on blood pressure.
Methods: We studied 5673 participants from the Prevention of Renal and Vascular End-Stage Disease(PREVEND) study. Urinary chloride(uCl) and sodium(uNa) were measured in two 24-hour collections. We used generalized-linear-regression to evaluate the relation of uCl and uNa with baseline blood pressure and Cox-proportional-hazards-analysis to assess the association with hypertension. Multicollinearity was assessed with Ridge regression.
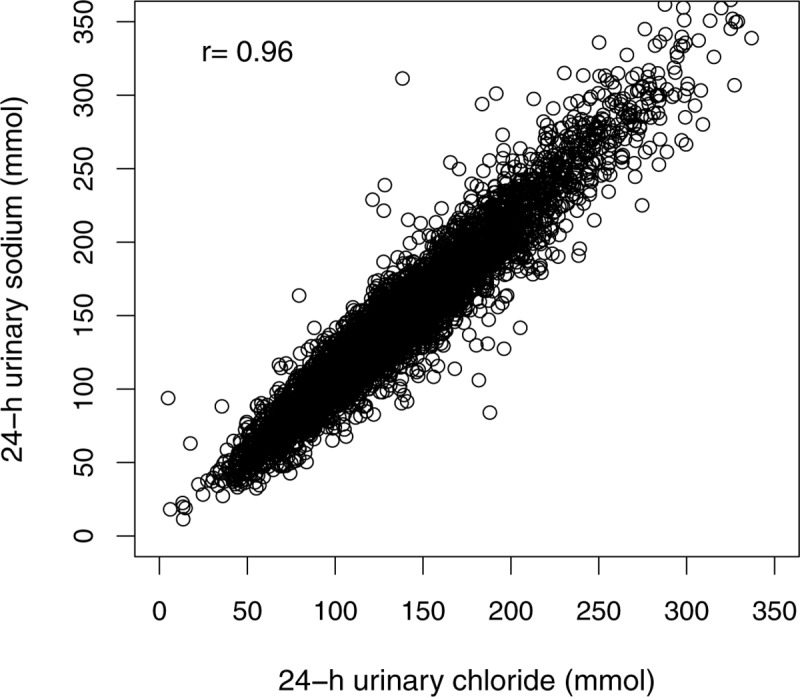
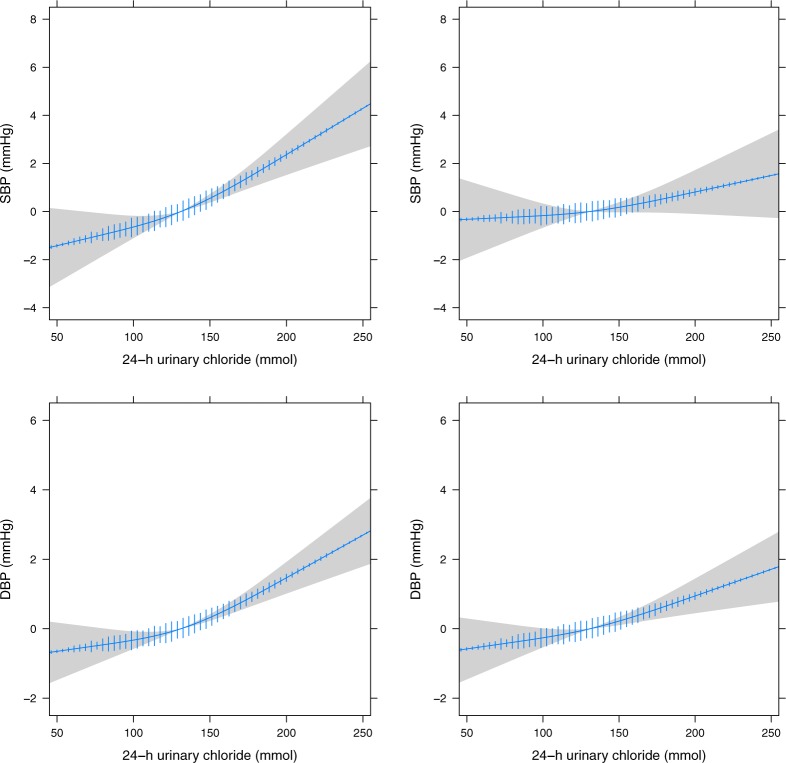
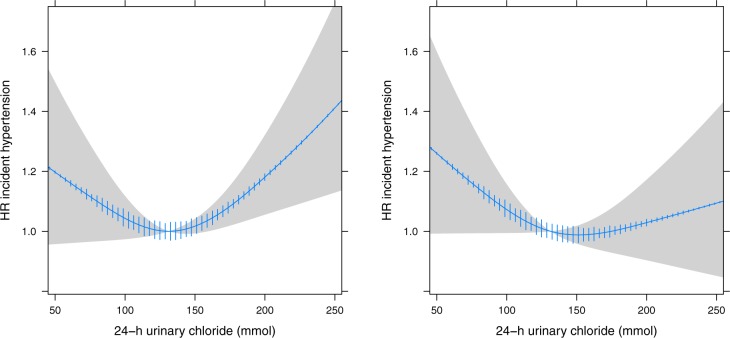
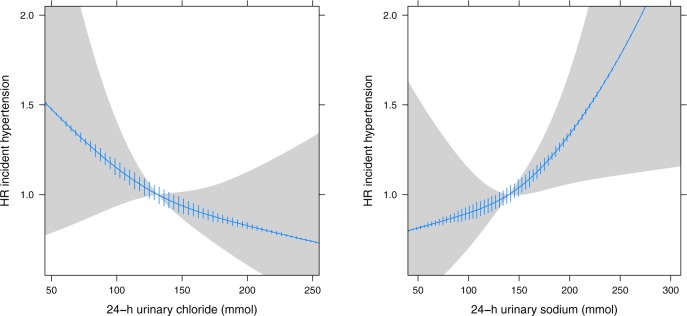
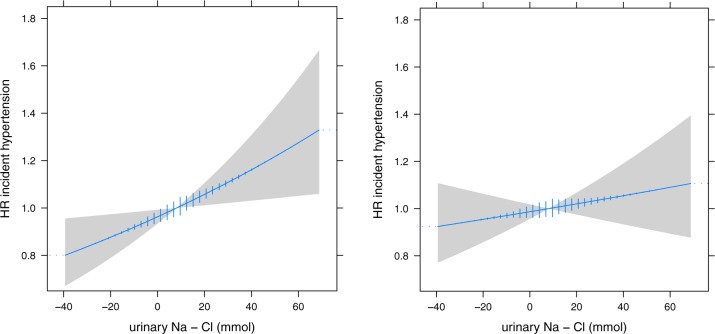
Results: Baseline 24-hour uCl was 135±39mmol and uNa was 144±54mmol. The correlation between uCl and uNa was high (Pearson's r = 0.96). UCl and uNa had similar non-significant positive and linear associations with blood pressure. In 3515 normotensive patients, 1021 patients developed hypertension during a median follow-up of 7.4 years. UCl and uNa had a comparable but non-significant J-shaped effect on the risk of hypertension. Adding both uCl and uNa to the same model produced instability, demonstrated by Ridge coefficients that converged or changed sign. The single index of uNa minus uCl showed a non-significant higher risk of hypertension of 2% per 10mmol/24-hour difference (HR1.02, 95%CI 0.98-1.06).
Conclusion: UCl and uNa had similar positive but non-significant associations with blood pressure and risk of hypertension and their effects could not be disentangled. Hence, the alleged adverse effects of high salt intake could be due to sodium, chloride or both. This encourages further study into the effect of chloride in order to complement dietary recommendations currently focused on sodium alone.
Conflict of interest statement
This work was supported by a research grant from Astellas to JvdL and MBR. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Urine chloride trajectory and relationship with diuretic response in acute heart failure.ESC Heart Fail. 2025 Feb;12(1):133-141. doi: 10.1002/ehf2.15054. Epub 2024 Oct 22. ESC Heart Fail. 2025. PMID: 39438405 Free PMC article.
-
Estimation of salt intake by urinary sodium excretion in a Portuguese adult population and its relationship to arterial stiffness.Rev Port Cardiol. 2006 Sep;25(9):801-17. Rev Port Cardiol. 2006. PMID: 17100171 English, Portuguese.
-
Urinary potassium excretion and risk of developing hypertension: the prevention of renal and vascular end-stage disease study.Hypertension. 2014 Oct;64(4):769-76. doi: 10.1161/HYPERTENSIONAHA.114.03750. Epub 2014 Jul 21. Hypertension. 2014. PMID: 25047575
-
Reducing salt intake for prevention of cardiovascular disease--times are changing.Adv Chronic Kidney Dis. 2015 Mar;22(2):108-15. doi: 10.1053/j.ackd.2014.12.002. Adv Chronic Kidney Dis. 2015. PMID: 25704347 Review.
-
Impact of Salt Intake on the Pathogenesis and Treatment of Hypertension.Adv Exp Med Biol. 2017;956:61-84. doi: 10.1007/5584_2016_147. Adv Exp Med Biol. 2017. PMID: 27757935 Review.
Cited by
-
Clues and new evidences in arterial hypertension: unmasking the role of the chloride anion.Pflugers Arch. 2022 Jan;474(1):155-176. doi: 10.1007/s00424-021-02649-5. Epub 2021 Dec 30. Pflugers Arch. 2022. PMID: 34966955 Review.
-
Electrolytes and Cardiovascular Disease Risk.Am J Lifestyle Med. 2020 May 8;14(4):361-365. doi: 10.1177/1559827620915708. eCollection 2020 Jul-Aug. Am J Lifestyle Med. 2020. PMID: 33281514 Free PMC article. Review.
-
Electrochemical Sensing of Urinary Chloride Ion Concentration for Near Real-Time Monitoring.Biosensors (Basel). 2023 Feb 28;13(3):331. doi: 10.3390/bios13030331. Biosensors (Basel). 2023. PMID: 36979543 Free PMC article.
References
-
- Cook NR, Cutler JA, Obarzanek E, Buring JE, Rexrode KM, Kumanyika SK, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: Observational follow-up of the trials of hypertension prevention (TOHP). Br Med J. 2007;334: 885–888. 10.1136/bmj.39147.604896.55 - DOI - PMC - PubMed
-
- Ambard L; Beaujard E. Causes de l’hypertension arterielle. Arch Gen Med. 1904;1: 520–533.
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial h. J Hypertens. 2018;36: 1953–2041. 10.1097/HJH.0000000000001940 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
