

Divergent mutational processes distinguish hypoxic and normoxic tumours
- PMID: 32024819
- PMCID: PMC7002770
- DOI: 10.1038/s41467-019-14052-x
Divergent mutational processes distinguish hypoxic and normoxic tumours
Erratum in
-
Author Correction: Divergent mutational processes distinguish hypoxic and normoxic tumours.Nat Commun. 2022 Dec 8;13(1):7569. doi: 10.1038/s41467-022-32339-4. Nat Commun. 2022. PMID: 36481612 Free PMC article. No abstract available.
Abstract
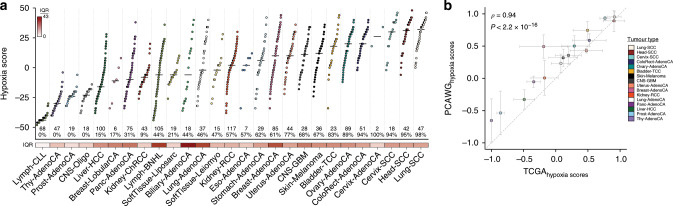
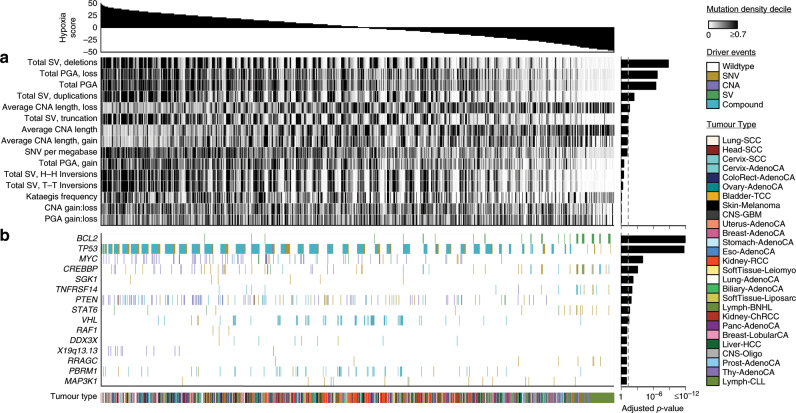
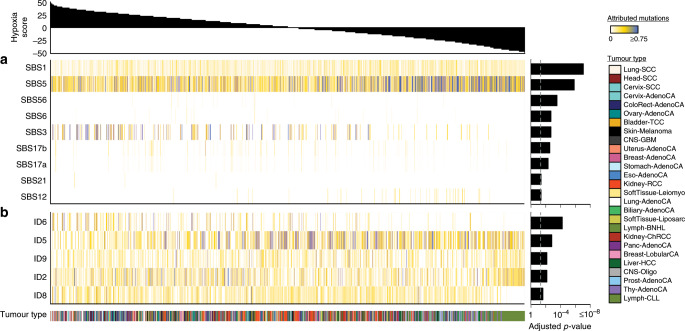
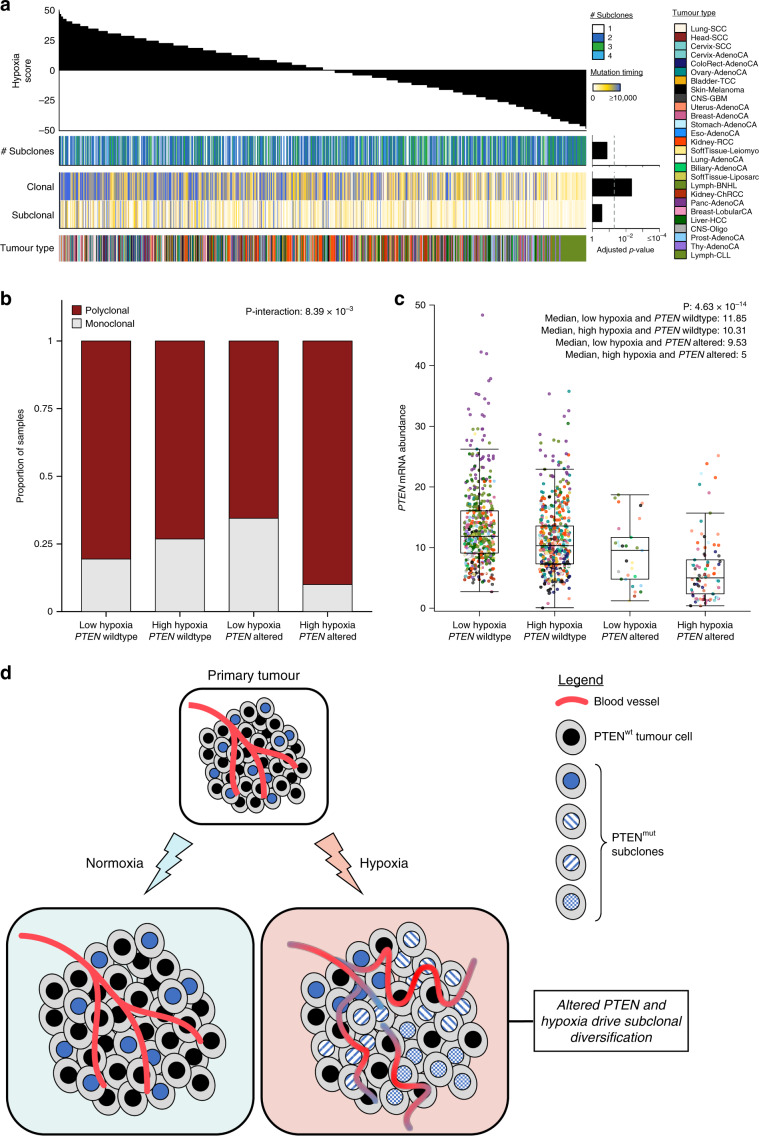
Many primary tumours have low levels of molecular oxygen (hypoxia), and hypoxic tumours respond poorly to therapy. Pan-cancer molecular hallmarks of tumour hypoxia remain poorly understood, with limited comprehension of its associations with specific mutational processes, non-coding driver genes and evolutionary features. Here, as part of the ICGC/TCGA Pan-Cancer Analysis of Whole Genomes (PCAWG) Consortium, which aggregated whole genome sequencing data from 2658 cancers across 38 tumour types, we quantify hypoxia in 1188 tumours spanning 27 cancer types. Elevated hypoxia associates with increased mutational load across cancer types, irrespective of underlying mutational class. The proportion of mutations attributed to several mutational signatures of unknown aetiology directly associates with the level of hypoxia, suggesting underlying mutational processes for these signatures. At the gene level, driver mutations in TP53, MYC and PTEN are enriched in hypoxic tumours, and mutations in PTEN interact with hypoxia to direct tumour evolutionary trajectories. Overall, hypoxia plays a critical role in shaping the genomic and evolutionary landscapes of cancer.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
