

Combined technique with hydroxyapatite coated intramedullary nails in treatment of anterolateral bowing of congenital pseudarthrosis of tibia
- PMID: 32025131
- PMCID: PMC6997496
- DOI: 10.1016/j.jor.2019.11.017
Combined technique with hydroxyapatite coated intramedullary nails in treatment of anterolateral bowing of congenital pseudarthrosis of tibia
Abstract
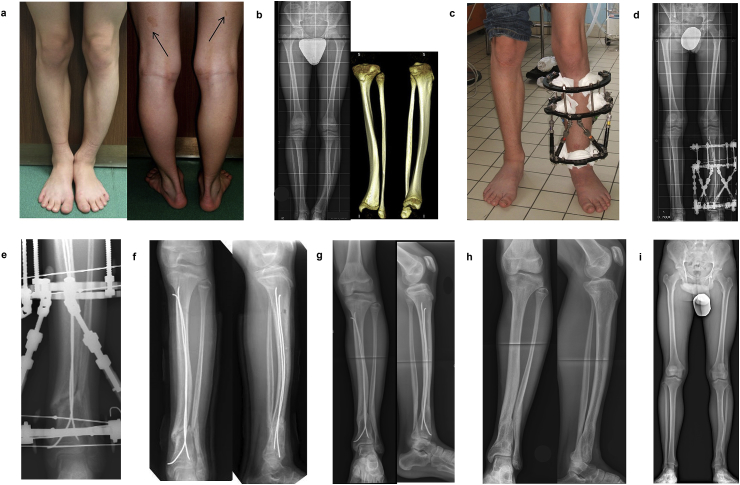
Purpose: The goal of this study is to evaluate the treatment outcomes of anterolateral bowing and residual deformities of distal tibia in patients with CPT using circular external fixation and hydroxyapatite coated flexible intramedullary nailing without excision of affected part of tibia.
Patients and methods: Six patients (4 boys and 2 girls, mean age 12.4 ± 4.1 years) were included in the study. Mean follow-up is 2.1 years. In 4 patients with early onset of disease initial surgical treatment (at age of 5-8 years) was dysplastic zone or pseudarthrosis resection with proximal metaphyseal osteotomy for bone transport. Children with unbroken bowed tibia (2 cases of type II according to Crawford classification) had no previous surgery. Neurofibromatosis type I was diagnosed in 4 cases. Surgical technique for residual deformity correction consisted of percutaneous osteotomy, application of circular external frame and composite hydroxyapatite-coated intramedullary nailing.
Results: Mean external fixation time was 95.3 ± 17.5 days. All patients never get fractured after frame removal. At the present time, they are considered to be healed, in 2.1 years, in average, without fractures or deformity recurrence. Mean lower limb length discrepancy varied from 2 to 10 mm at the latest follow-up control. After realignment procedure, patients didn't require additional surgery but one. Intramedullary nails were removed in two years after deformity correction for individual reason.
Conclusion: Correction of anterolateral bowing or residual deformity in children with CPT is indicated. Association of external fixation with intramedullary nailing/rodding left in situ after frame removal ensure stability and accuracy of deformity correction. Biological methods of stimulation of bone formation in dysplastic zone are obligatory to ensure bone union. Intramedullary nailing with composite hydroxyapatite-coated surface provides mechanical and biological advantages in patients with CPT.
Keywords: Flexible intramedullary nailing; Hydroxyapatite; congenital pseudarthrosis of tibia.
© 2019 Professor P K Surendran Memorial Education Foundation. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Andersen K.S. Occurrence of congenital tibial pseudoarthrosis in Denmark 1940–1965. Nord Med. 1971;86:1395. - PubMed
-
- Pannier S. Congenital pseudarthrosis of the tibia. Orthop Traumatol: Surg Res. 2011;97:750–761. - PubMed
-
- Leskelä H.-V., Kuorilehto T., Risteli J. Congenital pseudarthrosis of neurofibromatosis type 1: impaired osteoblast differentiation and function and altered NF1 gene expression. Bone. 2009;44:243–250. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
