

Antimicrobial de-escalation as part of antimicrobial stewardship in intensive care: no simple answers to simple questions-a viewpoint of experts
- PMID: 32025778
- PMCID: PMC7224113
- DOI: 10.1007/s00134-019-05871-z
Antimicrobial de-escalation as part of antimicrobial stewardship in intensive care: no simple answers to simple questions-a viewpoint of experts
Abstract
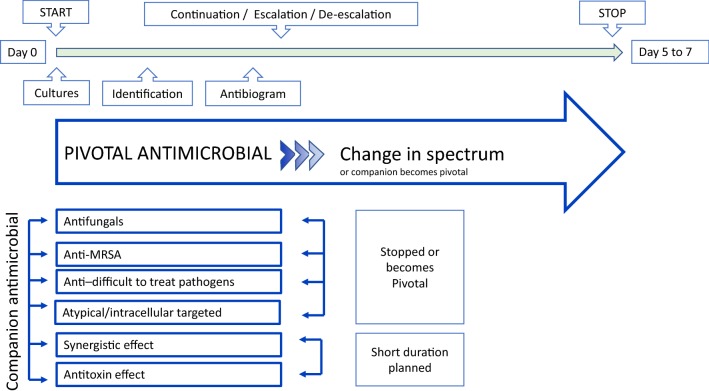
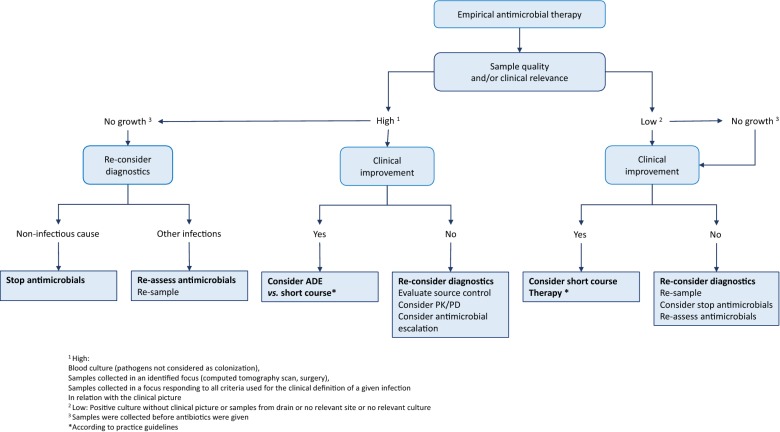
Antimicrobial de-escalation (ADE) is defined as the discontinuation of one or more components of combination empirical therapy, and/or the change from a broad-spectrum to a narrower spectrum antimicrobial. It is most commonly recommended in the intensive care unit (ICU) patient who is treated with broad-spectrum antibiotics as a strategy to reduce antimicrobial pressure of empirical broad-spectrum therapy and prevent antimicrobial resistance, yet this has not been convincingly demonstrated in a clinical setting. Even if it appears beneficial, ADE may have some unwanted side effects: it has been associated with prolongation of antimicrobial therapy and could inappropriately be used as a justification for unrestricted broadness of empirical therapy. Also, exposing a patient to multiple, sequential antimicrobials could have unwanted effects on the microbiome. For these reasons, ADE has important shortcomings to be promoted as a quality indicator for appropriate antimicrobial use in the ICU. Despite this, ADE clearly has a role in the management of infections in the ICU. The most appropriate use of ADE is in patients with microbiologically confirmed infections requiring longer antimicrobial therapy. ADE should be used as an integral part of an ICU antimicrobial stewardship approach in which it is guided by optimal specimen quality and relevance. Rapid diagnostics may further assist in avoiding unnecessary initiation of broad-spectrum therapy, which in turn will decrease the need for subsequent ADE.
Keywords: Antibiotic; Antimicrobial; Antimicrobial resistance; Antimicrobial stewardship; De-escalation; Sepsis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Antimicrobial de-escalation is part of appropriate antibiotic usage in ICU.Intensive Care Med. 2020 May;46(5):1039-1042. doi: 10.1007/s00134-020-05951-5. Epub 2020 Feb 20. Intensive Care Med. 2020. PMID: 32077998 Free PMC article. No abstract available.
References
-
- Tabah A, Cotta MO, Garnacho-Montero J, Schouten J, Roberts JA, Lipman J, Tacey M, Timsit JF, Leone M, Zahar JR, De Waele JJ. A systematic review of the definitions, determinants, and clinical outcomes of antimicrobial de-escalation in the intensive care unit. Clin Infect Dis. 2016;62:1009–1017. doi: 10.1093/cid/civ1199. - DOI - PubMed
-
- Tabah A, Bassetti M, Kollef MH, Zahar JR, Paiva JA, Timsit JF, Roberts J, Schouten J, Giamarellou H, Rello J, De Waele J, Shorr A, Leone M, Poulakou G, Depuydt P, Garnacho-Montero J. Antimicrobial de-escalation in critically ill patients: a position statement from a task force of the European Society of Intensive Care Medicine (ESICM) and European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Critically Ill Patients Study Group (ESGCIP) Intensive Care Med. 2019 doi: 10.1007/s00134-019-05866-w. - DOI - PubMed
-
- Rello J, Paiva JA, Baraibar J, Barcenilla F, Bodi M, Castander D, Correa H, Diaz E, Garnacho J, Llorio M, Rios M, Rodriguez A, Solé-Violán J. International conference for the development of consensus on the diagnosis and treatment of ventilator-associated pneumonia. Chest. 2001;120:955–970. doi: 10.1378/chest.120.3.955. - DOI - PubMed
-
- De Waele JJ, Akova M, Antonelli M, Canton R, Carlet J, De Backer D, Dimopoulos G, Garnacho-Montero J, Kesecioglu J, Lipman J, Mer M, Paiva JA, Poljak M, Roberts JA, Rodriguez Bano J, Timsit JF, Zahar JR, Bassetti M. Antimicrobial resistance and antibiotic stewardship programs in the ICU: insistence and persistence in the fight against resistance. A position statement from ESICM/ESCMID/WAAAR round table on multi-drug resistance. Intensive Care Med. 2018;44:189–196. doi: 10.1007/s00134-017-5036-1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
