

Airway tapering: an objective image biomarker for bronchiectasis
- PMID: 32025831
- PMCID: PMC7160094
- DOI: 10.1007/s00330-019-06606-w
Airway tapering: an objective image biomarker for bronchiectasis
Abstract
Purpose: To estimate airway tapering in control subjects and to assess the usability of tapering as a bronchiectasis biomarker in paediatric populations.
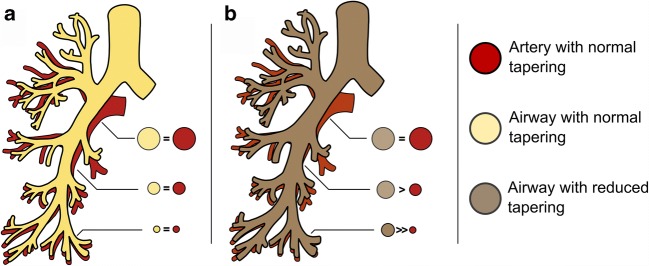
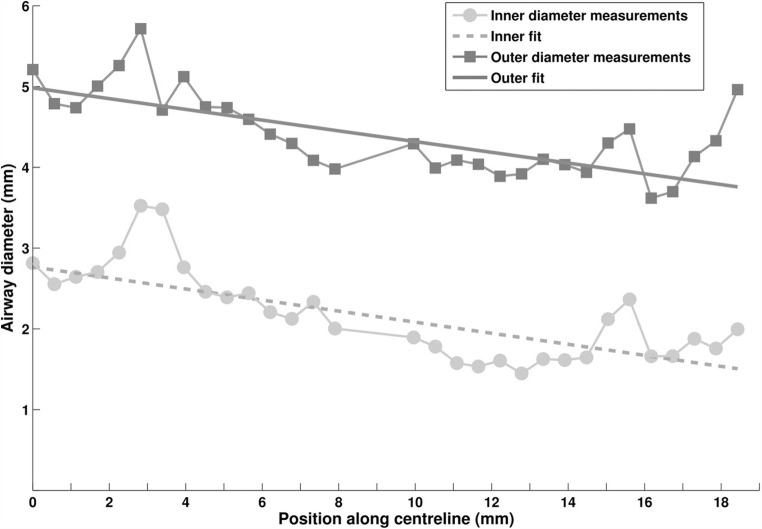
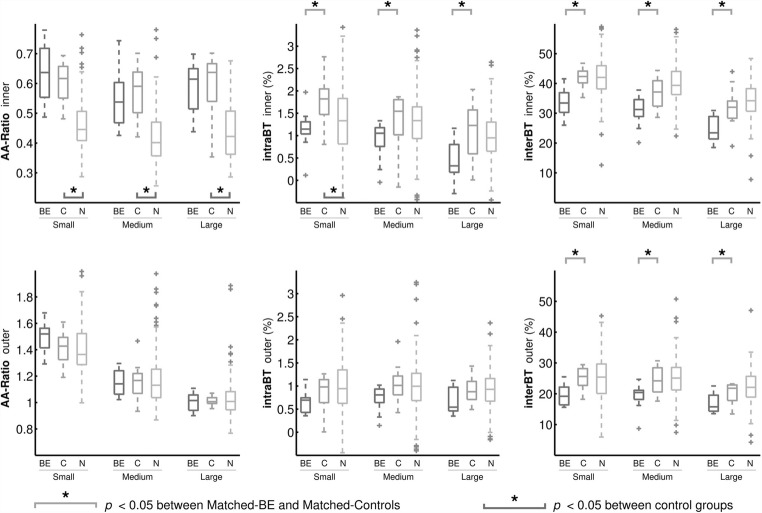
Methods: Airway tapering values were semi-automatically quantified in 156 children with control CTs collected in the Normal Chest CT Study Group. Airway tapering as a biomarker for bronchiectasis was assessed on spirometer-guided inspiratory CTs from 12 patients with bronchiectasis and 12 age- and sex-matched controls. Semi-automatic image analysis software was used to quantify intra-branch tapering (reduction in airway diameter along the branch), inter-branch tapering (reduction in airway diameter before and after bifurcation) and airway-artery ratios on chest CTs. Biomarkers were further stratified in small, medium and large airways based on three equal groups of the accompanying vessel size.
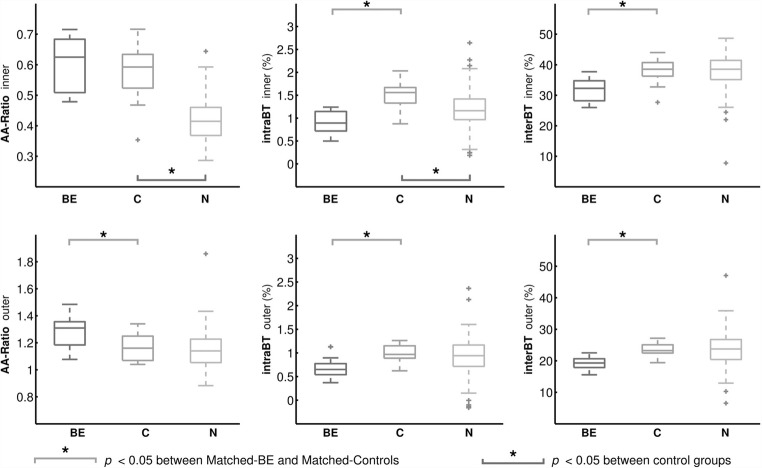
Results: Control subjects showed intra-branch tapering of 1% and inter-branch tapering of 24-39%. Subjects with bronchiectasis showed significantly reduced intra-branch of 0.8% and inter-branch tapering of 19-32% and increased airway-artery ratios compared with controls (p < 0.01). Tapering measurements were significantly different between diseased and controls across all airway sizes. Difference in airway-artery ratio was only significant in small airways.
Conclusion: Paediatric normal values for airway tapering were established in control subjects. Tapering showed to be a promising biomarker for bronchiectasis as subjects with bronchiectasis show significantly less airway tapering across all airway sizes compared with controls. Detecting less tapering in larger airways could potentially lead to earlier diagnosis of bronchiectasis. Additionally, compared with the conventional airway-artery ratio, this novel biomarker has the advantage that it does not require pairing with pulmonary arteries.
Key points: • Tapering is a promising objective image biomarker for bronchiectasis that can be extracted semi-automatically and has good correlation with validated visual scoring methods. • Less airway tapering was observed in patients with bronchiectasis and can be observed sensitively throughout the bronchial tree, even in the more central airways. • Tapering values seemed to be less influenced by variety in scanning protocols and lung volume making it a more robust biomarker for bronchiectasis detection.
Keywords: Bronchi; Bronchiectasis; Image interpretation computer-assisted; Imaging three-dimensional; Multidetector computed tomography.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Newell J.D. (2008) Bronchiectasis. In: Boiselle PM, Lynch DA (Eds) CT of the Airways. Contemporary Medical Imaging. Humana Press
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
