

A Real-World Analysis of Patient Characteristics and Predictors of Hospitalization Among US Medicare Beneficiaries with Respiratory Syncytial Virus Infection
- PMID: 32026380
- PMCID: PMC7223753
- DOI: 10.1007/s12325-020-01230-3
A Real-World Analysis of Patient Characteristics and Predictors of Hospitalization Among US Medicare Beneficiaries with Respiratory Syncytial Virus Infection
Abstract
Introduction: Little has been published on respiratory syncytial virus (RSV) among Medicare patients at high risk (HR) of RSV complications due to age or comorbidity.
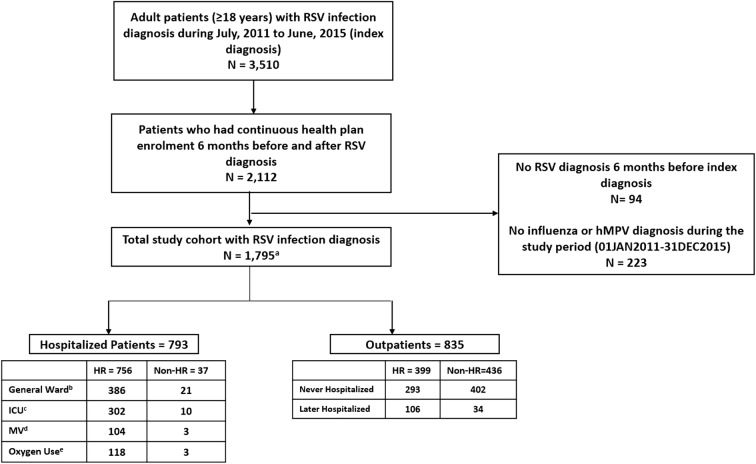
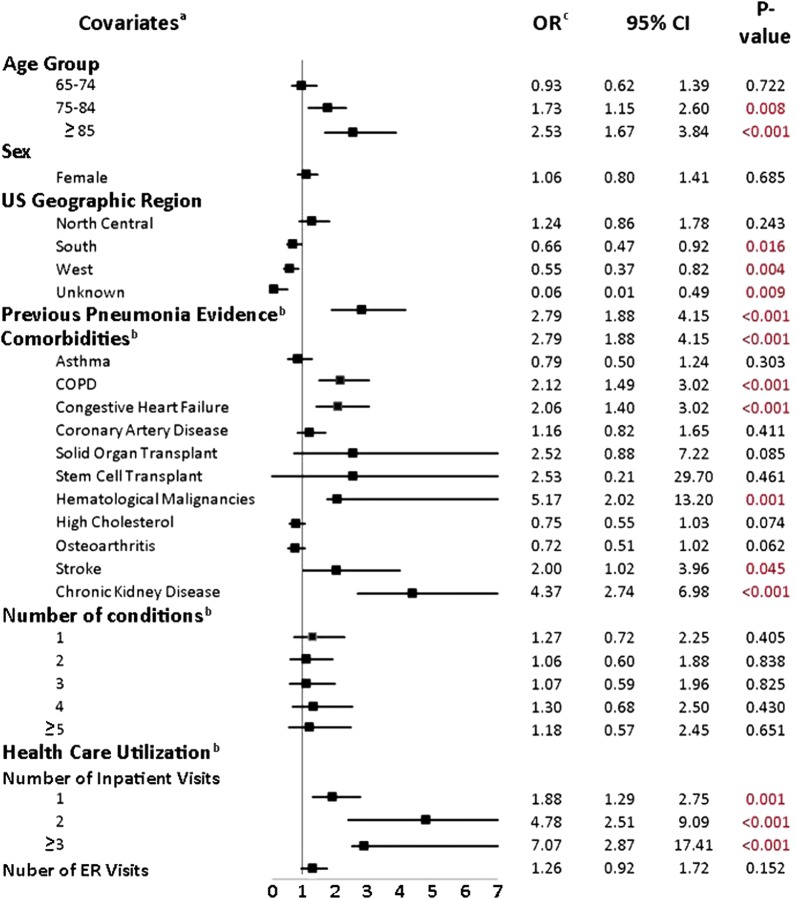
Methods: Adult patients (at least 18 years of age) with at least 1 diagnostic code for RSV were identified using the 5% US Medicare database from 2011 through 2015. Patients were required to have continuous health plan enrollment for 180 days pre- and 180 days post-RSV diagnosis (baseline and follow-up periods, respectively). HR was defined as diagnosis of chronic lung disease, congestive heart failure, or weakened immune system for 180 days during the baseline period. Patients were categorized as initially hospitalized if hospitalized within 1 day of RSV diagnosis. Logistic regression models were developed to determine predictors of initial hospitalization. Healthcare utilization and costs for 180 days pre- and post-RSV diagnosis were compared.
Results: The study included 756 HR patients who were initially hospitalized with RSV diagnoses. Among these, 61.7% were diagnosed in the emergency department vs 15.3% in a physician's office, with hypertension (76.3%), chronic obstructive pulmonary disease (COPD) (53.7%), and high cholesterol (52.0%) observed as the most prevalent comorbidities. Of these, COPD, congestive heart failure, chronic kidney disease, and previous evidence of pneumonia were significant predictors of hospitalization. Other significant predictors of hospitalization included older age, hematological malignancies, stroke, and baseline healthcare resource use. Among both HR and non-HR hospitalized patients, there was a significant increase in healthcare resource utilization following hospitalization, including the number of inpatient admissions and longer hospital stays post-RSV diagnosis. The total mean all-cause healthcare costs among HR hospitalized patients increased by $9210 per patient (p < 0.0001) post-RSV diagnosis.
Conclusion: Hospitalized Medicare beneficiaries with RSV infections pose a significant healthcare burden as compared with non-hospitalized patients, mainly driven by higher comorbidity, higher likelihood of multiple inpatient admissions, and costly medical interventions.
Keywords: Infectious disease; Medicare; Predictors of hospitalization; Respiratory syncytial virus.
Figures

References
-
- RSV in Older Adults and Adults with Chronic Medical Conditions|CDC [Internet]. Cdc.gov. 2019. https://www.cdc.gov/rsv/high-risk/older-adults.html. Accessed 6 Aug 2019.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
