

Cost Effectiveness of Antenatal Lifestyle Interventions for Preventing Gestational Diabetes and Hypertensive Disease in Pregnancy
- PMID: 32026397
- PMCID: PMC7426355
- DOI: 10.1007/s41669-020-00197-9
Cost Effectiveness of Antenatal Lifestyle Interventions for Preventing Gestational Diabetes and Hypertensive Disease in Pregnancy
Abstract
Background: Lifestyle interventions (diet, physical activity and/or behavioural) to optimise gestational weight gain can prevent adverse maternal outcomes such as gestational diabetes, pre-eclampsia and caesarean section.
Objective: We aimed to model the cost effectiveness of lifestyle interventions during pregnancy on reducing adverse maternal outcomes.
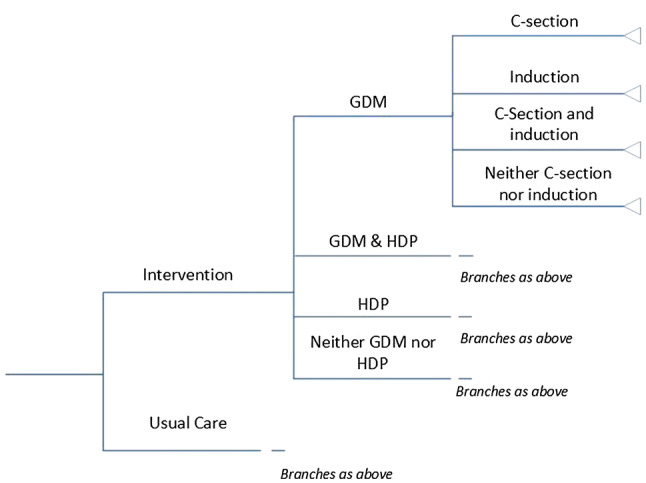
Methods: Decision tree modelling was used to determine the cost effectiveness of lifestyle interventions compared with usual care on preventing cases of gestational diabetes and hypertensive disease in pregnancy. Participants were pregnant women receiving routine antenatal care in secondary and tertiary care hospitals. The main outcome measures were cases of gestational diabetes and/or hypertensive disease in pregnancy prevented, costs, and incremental cost-effectiveness ratios. Analysis was conducted from the perspective of the Australian healthcare system, with a time horizon of early pregnancy to discharge after birth.
Results: Women in the intervention group were 2.25% less likely to have gestational diabetes and/or hypertensive disease in pregnancy (9.53%) compared with the control group (11.78%). Intervention costs were Australian dollars (AUD) 228 per person. Costs were AUD33 per person higher in the intervention group (AUD8281) than the control group (AUD8248). The incremental cost-effectiveness ratio was AUD1470 per case prevented. Sensitivity analysis showed that base-case results were robust. In the probabilistic sensitivity analysis, 44.8% of data points fell within the north-east quadrant, and 52.2% in the south-east quadrant (cost saving), with a 95% confidence interval ranging from AUD - 50,018 to 32,779 per case prevented.
Conclusions: While there is no formally accepted cost-effectiveness threshold for willingness-to-pay to prevent an adverse maternal event, the cost per person receiving a lifestyle intervention compared with controls was close to neutral, and therefore likely to be cost effective. Exploration of the cost effectiveness of different lifestyle delivery modes across various models of antenatal care is now required. Future cost-effectiveness studies should investigate longer time horizons, quality-adjusted life-years and productivity loss.
Trial registration: Not applicable.
Conflict of interest statement
Cate Bailey, Helen Skouteris, Cheryce L. Harrison, Jacqueline Boyle, Rebeccah Bartlett, Briony Hill, Shakila Thangaratinam, Helena Teede, and Zanfina Ademi declare they have no conflicts of interest.
Figures


References
-
- World Health Organization. Health topics: obesity. 2018. http://www.who.int/topics/obesity/en/. Accessed 20 Feb 2018.
-
- Institute of Medicine and National Research Council Committee to Reexamine IOM Pregnancy Weight Guidelines . Re-examining IOM Pregnancy Weight Guidelines. In: Rasmussen KM, Yaktine AL, editors. Weight gain during pregnancy: reexamining the guidelines. Washington, DC: National Academies Press; 2009. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
