

Association of Maximal Extent of Resection of Contrast-Enhanced and Non-Contrast-Enhanced Tumor With Survival Within Molecular Subgroups of Patients With Newly Diagnosed Glioblastoma
- PMID: 32027343
- PMCID: PMC7042822
- DOI: 10.1001/jamaoncol.2019.6143
Association of Maximal Extent of Resection of Contrast-Enhanced and Non-Contrast-Enhanced Tumor With Survival Within Molecular Subgroups of Patients With Newly Diagnosed Glioblastoma
Erratum in
-
Error in Institution Name in the Text.JAMA Oncol. 2020 Mar 1;6(3):444. doi: 10.1001/jamaoncol.2020.0360. JAMA Oncol. 2020. PMID: 32163171 Free PMC article. No abstract available.
Abstract
Importance: Per the World Health Organization 2016 integrative classification, newly diagnosed glioblastomas are separated into isocitrate dehydrogenase gene 1 or 2 (IDH)-wild-type and IDH-mutant subtypes, with median patient survival of 1.2 and 3.6 years, respectively. Although maximal resection of contrast-enhanced (CE) tumor is associated with longer survival, the prognostic importance of maximal resection within molecular subgroups and the potential importance of resection of non-contrast-enhanced (NCE) disease is poorly understood.
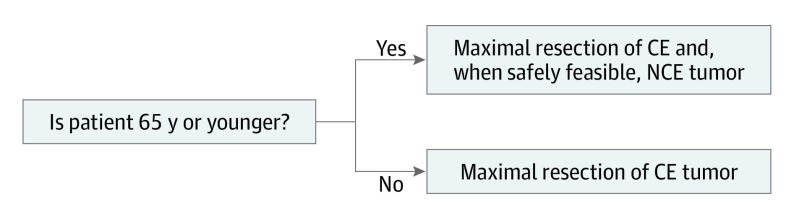
Objective: To assess the association of resection of CE and NCE tumors in conjunction with molecular and clinical information to develop a new road map for cytoreductive surgery.
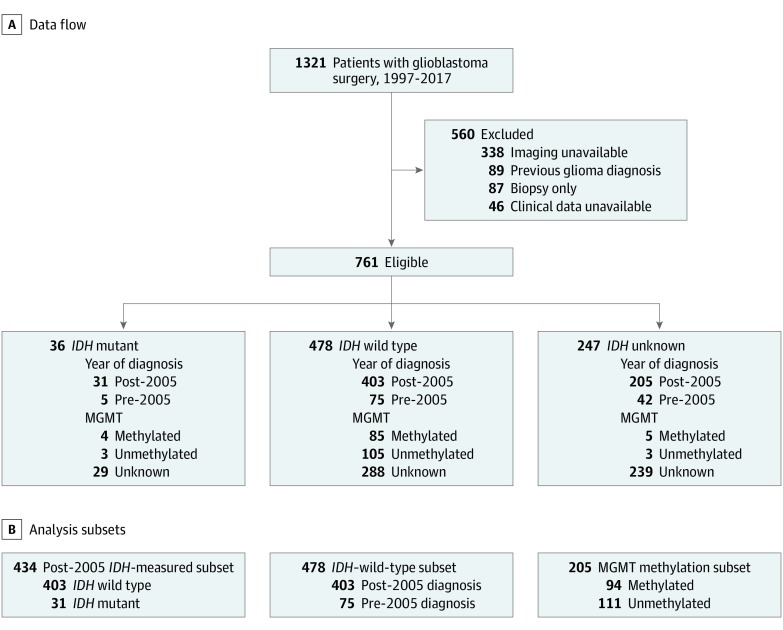
Design, setting, and participants: This retrospective, multicenter cohort study included a development cohort from the University of California, San Francisco (761 patients diagnosed from January 1, 1997, through December 31, 2017, with 9.6 years of follow-up) and validation cohorts from the Mayo Clinic (107 patients diagnosed from January 1, 2004, through December 31, 2014, with 5.7 years of follow-up) and the Ohio Brain Tumor Study (99 patients with data collected from January 1, 2008, through December 31, 2011, with a median follow-up of 10.9 months). Image accessors were blinded to patient groupings. Eligible patients underwent surgical resection for newly diagnosed glioblastoma and had available survival, molecular, and clinical data and preoperative and postoperative magnetic resonance images. Data were analyzed from November 15, 2018, to March 15, 2019.
Main outcomes and measures: Overall survival.
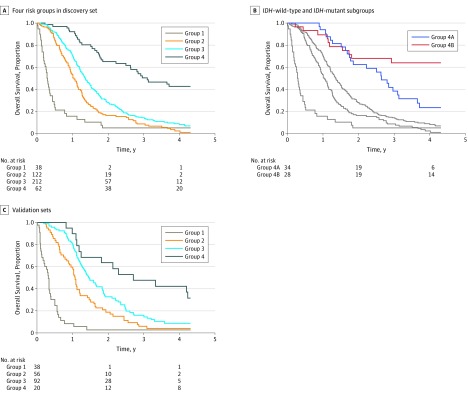
Results: Among the 761 patients included in the development cohort (468 [61.5%] men; median age, 60 [interquartile range, 51.6-67.7] years), younger patients with IDH-wild-type tumors and aggressive resection of CE and NCE tumors had survival similar to that of patients with IDH-mutant tumors (median overall survival [OS], 37.3 [95% CI, 31.6-70.7] months). Younger patients with IDH-wild-type tumors and reduction of CE tumor but residual NCE tumors fared worse (median OS, 16.5 [95% CI, 14.7-18.3] months). Older patients with IDH-wild-type tumors benefited from reduction of CE tumor (median OS, 12.4 [95% CI, 11.4-14.0] months). The results were validated in the 2 external cohorts. The association between aggressive CE and NCE in patients with IDH-wild-type tumors was not attenuated by the methylation status of the promoter region of the DNA repair enzyme O6-methylguanine-DNA methyltransferase.
Conclusions and relevance: This study confirms an association between maximal resection of CE tumor and OS in patients with glioblastoma across all subgroups. In addition, maximal resection of NCE tumor was associated with longer OS in younger patients, regardless of IDH status, and among patients with IDH-wild-type glioblastoma regardless of the methylation status of the promoter region of the DNA repair enzyme O6-methylguanine-DNA methyltransferase. These conclusions may help reassess surgical strategies for individual patients with newly diagnosed glioblastoma.
Conflict of interest statement
Figures

Comment in
-
A Common Rule for Resection of Glioblastoma in the Molecular Era.JAMA Oncol. 2020 Apr 1;6(4):503-504. doi: 10.1001/jamaoncol.2019.6384. JAMA Oncol. 2020. PMID: 32027348 No abstract available.
-
Extent of resection is important across glioblastoma molecular subtypes.Nat Rev Clin Oncol. 2020 May;17(5):275. doi: 10.1038/s41571-020-0344-8. Nat Rev Clin Oncol. 2020. PMID: 32080372 No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
