

Emerging 2019 Novel Coronavirus (2019-nCoV) Pneumonia
- PMID: 32027573
- PMCID: PMC7233366
- DOI: 10.1148/radiol.2020200274
Emerging 2019 Novel Coronavirus (2019-nCoV) Pneumonia
Erratum in
-
Emerging 2019 Novel Coronavirus (2019-nCoV) Pneumonia.Radiology. 2020 Dec;297(3):E346. doi: 10.1148/radiol.2020209021. Radiology. 2020. PMID: 33196374 Free PMC article. No abstract available.
Abstract
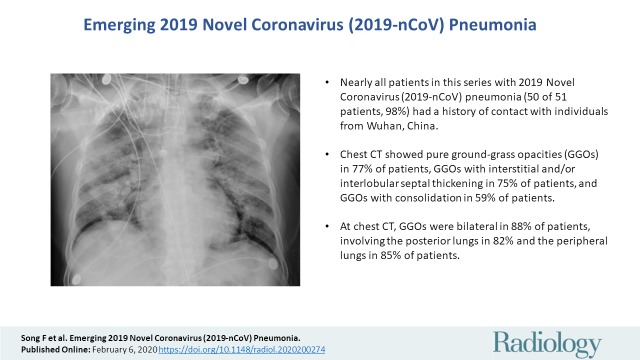
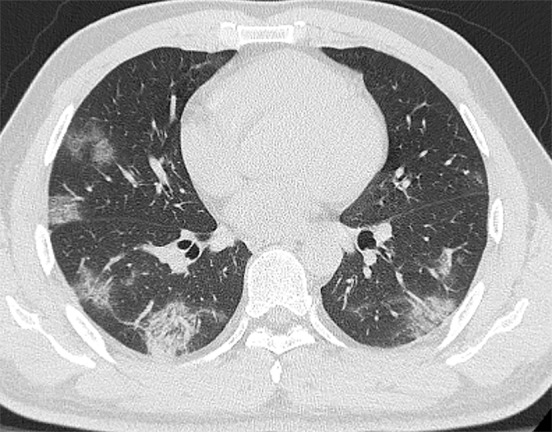
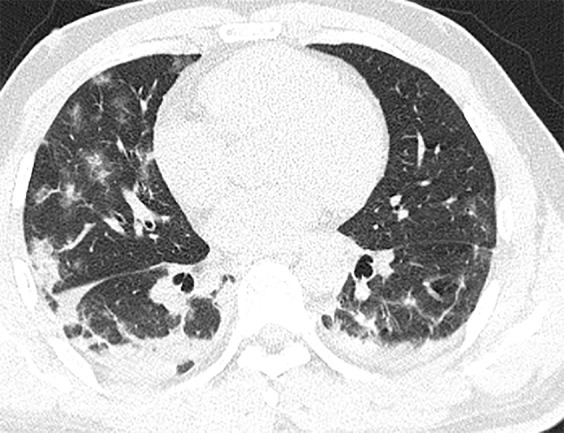
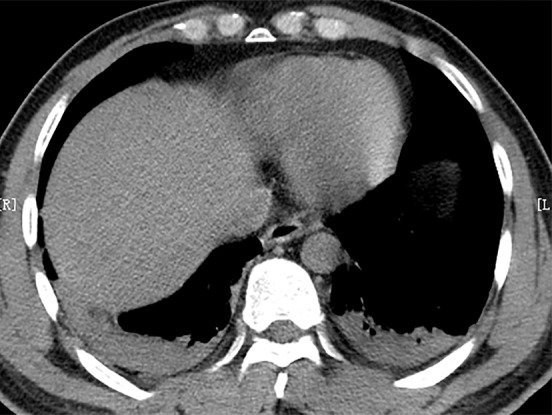
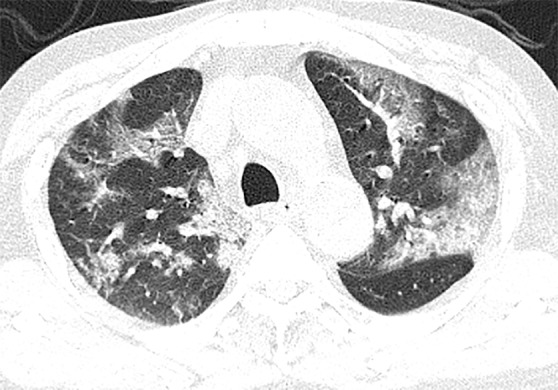
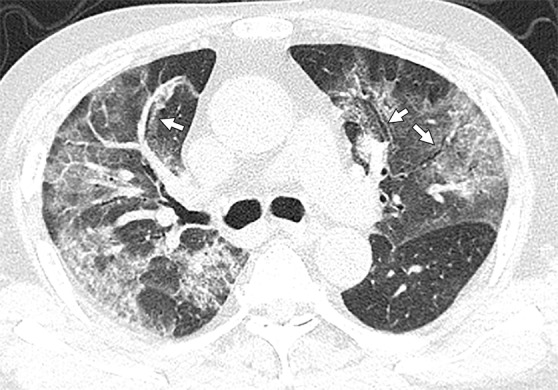
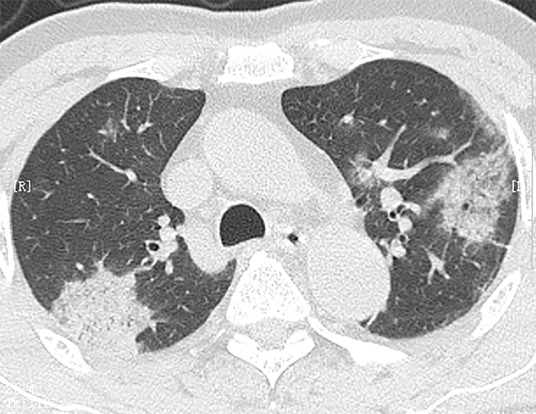
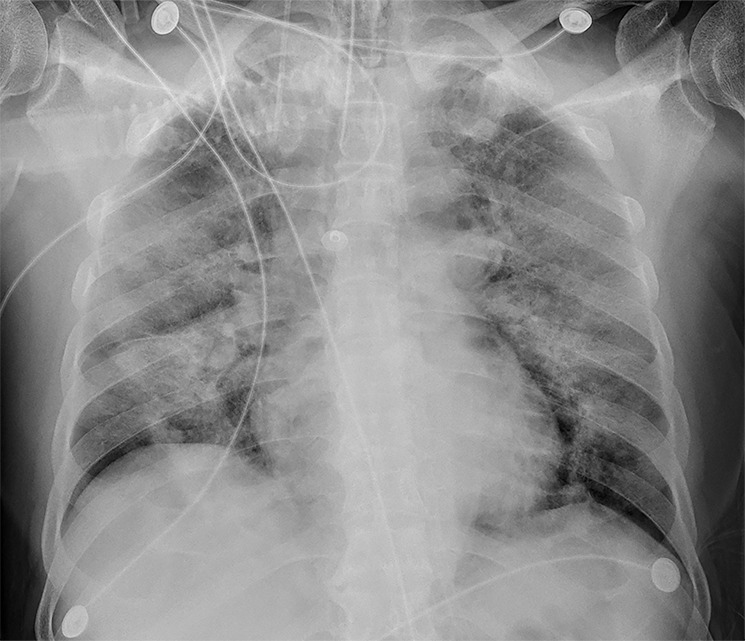
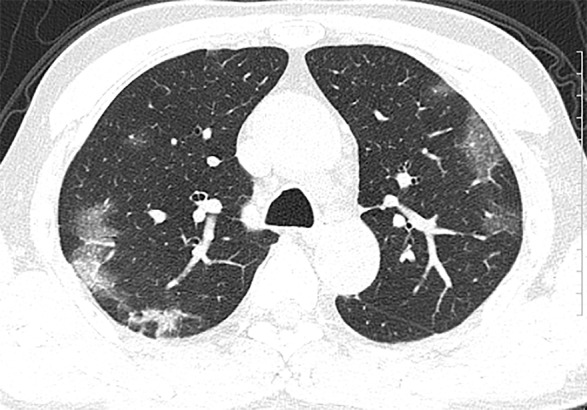
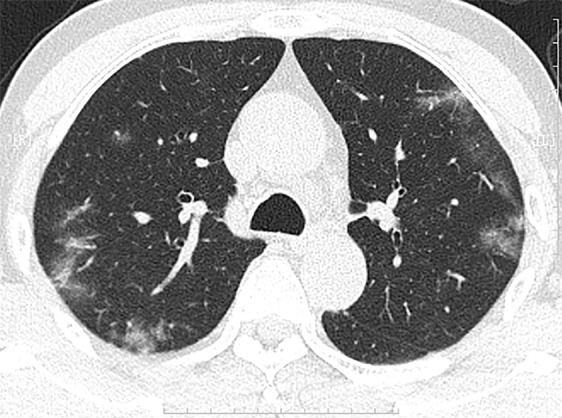
BackgroundThe chest CT findings of patients with 2019 Novel Coronavirus (2019-nCoV) pneumonia have not previously been described in detail.PurposeTo investigate the clinical, laboratory, and imaging findings of emerging 2019-nCoV pneumonia in humans.Materials and MethodsFifty-one patients (25 men and 26 women; age range 16-76 years) with laboratory-confirmed 2019-nCoV infection by using real-time reverse transcription polymerase chain reaction underwent thin-section CT. The imaging findings, clinical data, and laboratory data were evaluated.ResultsFifty of 51 patients (98%) had a history of contact with individuals from the endemic center in Wuhan, China. Fever (49 of 51, 96%) and cough (24 of 51, 47%) were the most common symptoms. Most patients had a normal white blood cell count (37 of 51, 73%), neutrophil count (44 of 51, 86%), and either normal (17 of 51, 35%) or reduced (33 of 51, 65%) lymphocyte count. CT images showed pure ground-glass opacity (GGO) in 39 of 51 (77%) patients and GGO with reticular and/or interlobular septal thickening in 38 of 51 (75%) patients. GGO with consolidation was present in 30 of 51 (59%) patients, and pure consolidation was present in 28 of 51 (55%) patients. Forty-four of 51 (86%) patients had bilateral lung involvement, while 41 of 51 (80%) involved the posterior part of the lungs and 44 of 51 (86%) were peripheral. There were more consolidated lung lesions in patients 5 days or more from disease onset to CT scan versus 4 days or fewer (431 of 712 lesions vs 129 of 612 lesions; P < .001). Patients older than 50 years had more consolidated lung lesions than did those aged 50 years or younger (212 of 470 vs 198 of 854; P < .001). Follow-up CT in 13 patients showed improvement in seven (54%) patients and progression in four (31%) patients.ConclusionPatients with fever and/or cough and with conspicuous ground-glass opacity lesions in the peripheral and posterior lungs on CT images, combined with normal or decreased white blood cells and a history of epidemic exposure, are highly suspected of having 2019 Novel Coronavirus (2019-nCoV) pneumonia.© RSNA, 2020.
Figures






Comment in
-
The use of radiological imaging alongside reverse transcriptase PCR in diagnosing novel coronavirus disease 2019: a narrative review.Future Microbiol. 2020 Jul;15:897-903. doi: 10.2217/fmb-2020-0098. Epub 2020 Jul 8. Future Microbiol. 2020. PMID: 32638613 Free PMC article.
References
-
- ProMED-mail. https://promedmail.org/promed-post/?id=6864153. Accessed January 7, 2020.
-
- World Health Organization . Novel coronavirus – Thailand (ex-China). http://www.who.int/csr/don/14-january-2020-novel-coronavirus-thailand/en/. Published January 14, 2020. Accessed January 19, 2020.
-
- World Health Organization . Novel coronavirus – Japan (ex-China). http://www.who.int/csr/don/17-january-2020-novel-coronavirus-japan-ex-ch.... Published January 17, 2020. Accessed January 19, 2020.
-
- World Health Organization . Novel coronavirus – Republic of Korea (ex-China). http://www.who.int/csr/don/21-january-2020-novel-coronavirus-republic-of.... Published January 21, 2020. Accessed January 23, 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
