

Cancer-Related Stroke: An Emerging Subtype of Ischemic Stroke with Unique Pathomechanisms
- PMID: 32027788
- PMCID: PMC7005348
- DOI: 10.5853/jos.2019.02278
Cancer-Related Stroke: An Emerging Subtype of Ischemic Stroke with Unique Pathomechanisms
Abstract
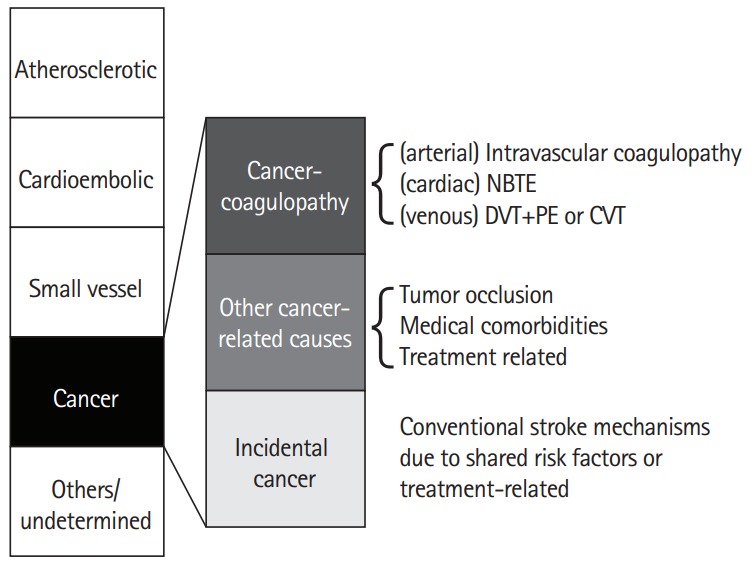
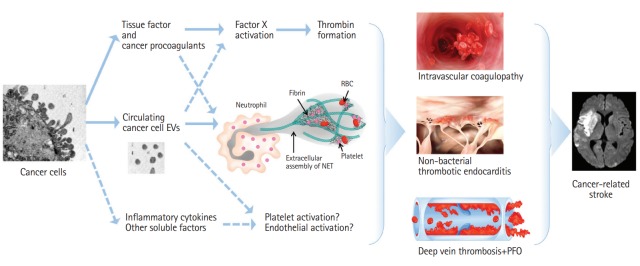
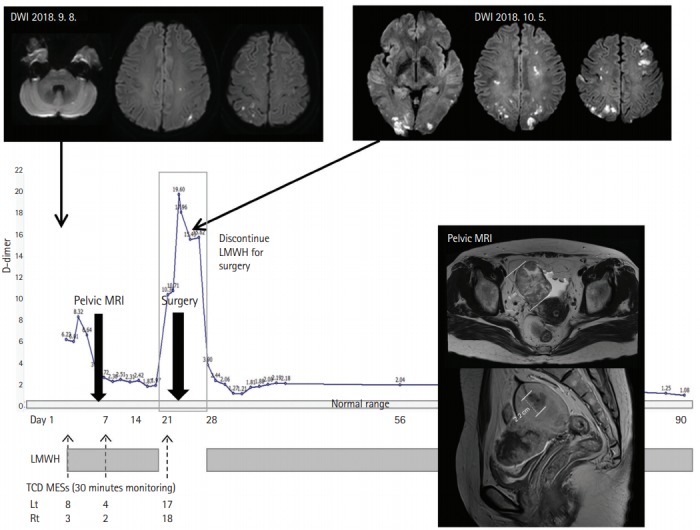
Systemic cancer and ischemic stroke are common conditions and two of the most frequent causes of death among the elderly. The association between cancer and stroke has been reported worldwide. Stroke causes severe disability for cancer patients, while cancer increases the risk of stroke. Moreover, cancer-related stroke is expected to increase due to advances in cancer treatment and an aging population worldwide. Because cancer and stroke share risk factors (such as smoking and obesity) and treatment of cancer can increase the risk of stroke (e.g., accelerated atherosclerosis after radiation therapy), cancer may accelerate conventional stroke mechanisms (i.e., atherosclerosis, small vessel disease, and cardiac thrombus). In addition, active cancer and chemotherapy may enhance thrombin generation causing stroke related to coagulopathy. Patients with stroke due to cancer-related coagulopathy showed the characteristics findings of etiologic work ups, D-dimer levels, and infarct patterns. In this review, we summarized the frequency of cancer-related stroke among patients with ischemic stroke, mechanisms of stroke with in cancer patients, and evaluation and treatment of cancer-related stroke. We discussed the possibility of cancer-related stroke as a stroke subtype, and presented the most recent discoveries in the pathomechanisms and treatment of stroke due to cancer-related coagulopathy.
Keywords: Cancer; Coagulopathy; Neoplasms; Stroke; Subtype; Thrombosis.
Figures
References
-
- Adams HP, Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute ischemic stroke: definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24:35–41. - PubMed
-
- Ay H, Furie KL, Singhal A, Smith WS, Sorensen AG, Koroshetz WJ. An evidence-based causative classification system for acute ischemic stroke. Ann Neurol. 2005;58:688–697. - PubMed
-
- Amarenco P, Bogousslavsky J, Caplan LR, Donnan GA, Hennerici MG. New approach to stroke subtyping: the A-SC-O (phenotypic) classification of stroke. Cerebrovasc Dis. 2009;27:502–508. - PubMed
-
- Marnane M, Duggan CA, Sheehan OC, Merwick A, Hannon N, Curtin D, et al. Stroke subtype classification to mechanismspecific and undetermined categories by TOAST, A-S-C-O, and causative classification system: direct comparison in the North Dublin population stroke study. Stroke. 2010;41:1579–1586. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
