

Neuroinflammation after Intracerebral Hemorrhage and Potential Therapeutic Targets
- PMID: 32027790
- PMCID: PMC7005353
- DOI: 10.5853/jos.2019.02236
Neuroinflammation after Intracerebral Hemorrhage and Potential Therapeutic Targets
Abstract
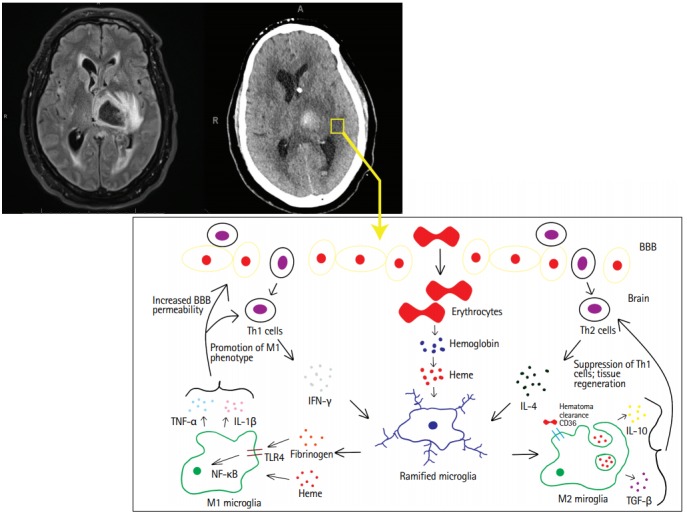
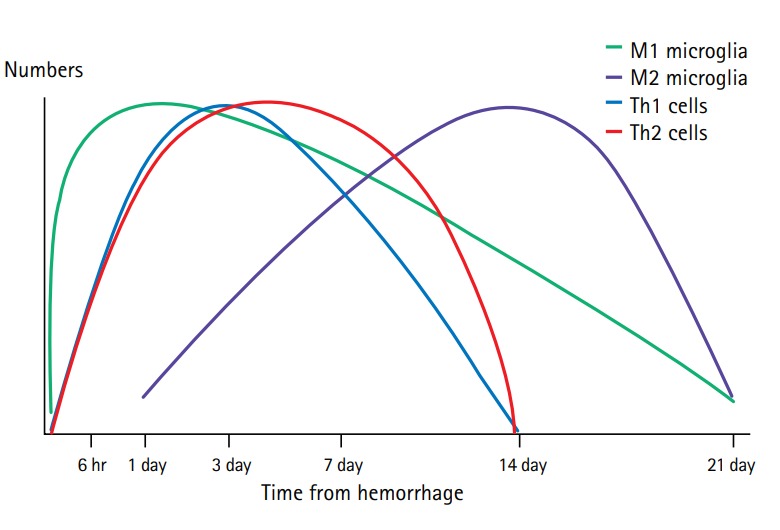
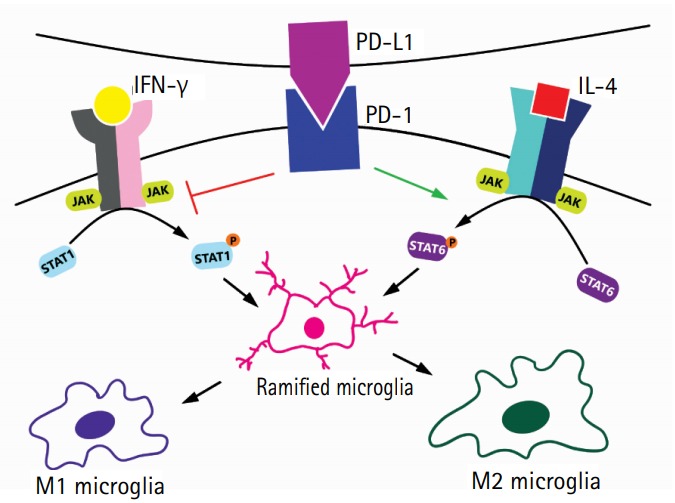
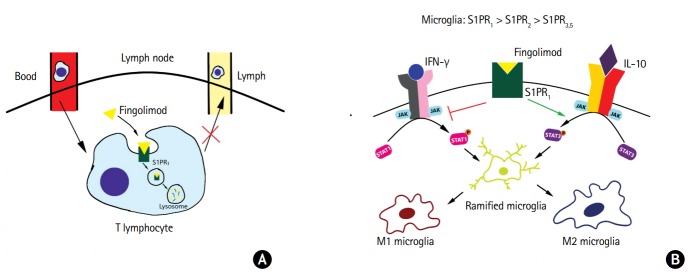
Spontaneous intracerebral hemorrhage (ICH) is a catastrophic illness causing significant morbidity and mortality. Despite advances in surgical technique addressing primary brain injury caused by ICH, little progress has been made treating the subsequent inflammatory cascade. Pre-clinical studies have made advancements identifying components of neuroinflammation, including microglia, astrocytes, and T lymphocytes. After cerebral insult, inflammation is initially driven by the M1 microglia, secreting cytokines (e.g., interleukin-1β [IL-1β] and tumor necrosis factor-α) that are involved in the breakdown of the extracellular matrix, cellular integrity, and the blood brain barrier. Additionally, inflammatory factors recruit and induce differentiation of A1 reactive astrocytes and T helper 1 (Th1) cells, which contribute to the secretion of inflammatory cytokines, augmenting M1 polarization and potentiating inflammation. Within 7 days of ICH ictus, the M1 phenotype coverts to a M2 phenotype, key for hematoma removal, tissue healing, and overall resolution of inflammation. The secretion of anti-inflammatory cytokines (e.g., IL-4, IL-10) can drive Th2 cell differentiation. M2 polarization is maintained by the secretion of additional anti-inflammatory cytokines by the Th2 cells, suppressing M1 and Th1 phenotypes. Elucidating the timing and trigger of the anti-inflammatory phenotype may be integral in improving clinical outcomes. A challenge in current translational research is the absence of an equivalent disease animal model mirroring the patient population and comorbid pathophysiologic state. We review existing data and describe potential therapeutic targets around which we are creating a bench to bedside translational research model that better reflects the pathophysiology of ICH patients.
Keywords: Cerebral hemorrhage; Fingolimod hydrochloride; Immunomodulation; Neuroinflammation; Programmed death-1; Stroke.
Figures
References
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9:167–176. - PubMed
-
- Writing Group Members, Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, et al. Heart disease and stroke statistics-2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- Qureshi AI, Suri MF, Nasar A, Kirmani JF, Ezzeddine MA, Divani AA, et al. Changes in cost and outcome among US patients with stroke hospitalized in 1990 to 1991 and those hospitalized in 2000 to 2001. Stroke. 2007;38:2180–2184. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
